Primary cardiac neoplasms are rare entities,[1, 2, 3] with an autopsy prevalence of 0.001-0.28%. The most common primary malignant tumor of the heart and pericardium is sarcoma.
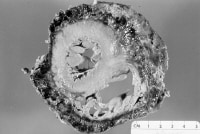 Angiosarcoma of the heart, with pericardial encasement by hemorrhagic tumor. Image courtesy of Dr. K. Marchant. NextPathophysiology
Angiosarcoma of the heart, with pericardial encasement by hemorrhagic tumor. Image courtesy of Dr. K. Marchant. NextPathophysiologyThe diagnosis of cardiac sarcoma is often not made preoperatively or even antemortem. It is overlooked because of the rarity of the lesion and the nonspecific nature of the symptoms and signs. Tumors that originate in the epicardium or pericardium and that lead to cardiac encasement may cause chest pain, hypotension, tachycardia, and malaise. Diminished cardiac sounds and a friction rub may be heard.
Cardiac tamponade (usually from a persistent and bloody pericardial effusion) may eventually cause intractable cardiac failure. Myocardial involvement may lead to refractory arrhythmias, heart block, heart failure, angina, or infarction. Endomyocardial masses cause valvular obstruction or insufficiency. Rarely, a pedunculated tumor causes an audible plop from tumor prolapse through a valve. Tumor fragments may embolize from the right side of the heart to the lungs and cause dyspnea or hemoptysis. Left-sided emboli may lead to cerebrovascular accidents, peripheral organ infarctions, seizures, and distant metastases. Local extension of tumors may cause signs and symptoms such as superior vena cava syndrome, hemoptysis, and dysphonia.
Several subtypes of primary cardiac sarcoma exist (ie, angiosarcoma,[4] rhabdomyosarcoma, mesothelioma, fibrosarcoma, malignant schwannoma), which occur in decreasing order of frequency in adults.[5, 6]
AngiosarcomaNearly 80% of cardiac angiosarcomas arise as mural masses in the right atrium. Typically, they completely replace the atrial wall and fill the entire cardiac chamber. They may invade adjacent structures (eg, vena cava, tricuspid valve).
These tumors are both symptomatic and rapidly fatal. Extensive pericardial spread and encasement of the heart often occur. Pericardial angiosarcoma (without myocardial involvement) occurs rarely.
RhabdomyosarcomaThis is the second most common primary cardiac sarcoma. It has been described in all age groups. No heart chamber is particularly favored. Diffuse pericardial spread is not often observed.
A myocardial component is nearly always present; valvular interference, only occasionally. Rhabdomyosarcoma is the most common form of cardiac sarcoma in children.
MesotheliomaThese tumors typically arise in the visceral or parietal pericardium and can spread to constrict the heart. They do not invade the underlying myocardium. Extensive local spread may lead to pleural, diaphragmatic, or peritoneal involvement.
Grossly, the tumor is firm and white, with both nodular and sheetlike growth. No age group has a particular predilection for these tumors. Interestingly, no etiologic association of pericardial mesotheliomas to asbestos exposure exists, in contrast to the more typical primary pleural mesotheliomas.
Fibrosarcoma and malignant fibrous histiocytomaThese whitish lesions have a firm texture and exhibit infiltrative growth patterns. No age or cardiac chamber predilection has been noted. However, cardiac valvular involvement is found in as many as 50% of lesions. Pericardial invasion rarely occurs.
Malignant schwannomaThis tumor is derived from peripheral nerve sheath tissue. Such tumors have a spatial association with the juxtacardiac position of the vagus nerve.
Metastatic cardiac sarcomaMetastases to the heart and pericardium are 40 times more common than primary cardiac tumors. In fact, an estimated 25% of patients who die from metastatic soft tissue sarcoma have cardiac metastases. No particular gross pattern of myocardial spread exists (ie, diffuse, nodular). In children, rhabdomyosarcoma is the most common type of sarcoma that metastasizes to the heart.
PreviousNextEpidemiologyFrequencyUnited StatesCardiac sarcoma occurs in less than 0.2% of decedents undergoing autopsy, both nationally and internationally.
InternationalFigures are the same as in the United States.
Mortality/MorbidityData on patients with primary cardiac sarcomas have shown that median survival is 6 months from the time of diagnosis.
SexSex predilection has not been defined for cardiac sarcoma.
AgeCardiac sarcomas can occur at any age; however, children have an increased rate of cardiac rhabdomyosarcomas.
PreviousProceed to Clinical Presentation , Cardiac Sarcoma











0 comments:
Post a Comment