Coronary artery atherosclerosis is the single largest killer of men and women in the United States. It is the principal cause of coronary artery disease (CAD), in which atherosclerotic changes are present within the walls of the coronary arteries.
Essential update: New European Society of Cardiology guidelines for stable CAD and CVD with diabetesThe European Society of Cardiology (ESC) released updated guidelines on the management of stable CAD.[1, 2] These guidelines note that microvascular angina and vasospasm are more common as causes of angina than previously believed, and they increase reliance on pretest probabilities (PTP) for stable CAD as well as discuss a larger role for modern imaging modalities (eg, cardiac magnetic resonance [CMR] imaging and coronary computed-tomography angiography [CCTA]).
Highlights of these new guidelines include the following[1, 2] :
PTP for a CAD diagnosis uses more contemporary data than those used in the Diamond and Forrester Chest Pain Prediction Rule: For example, in patients with suspected CAD using the new criteria, if the PTP is 85%), a diagnosis of CAD is established, and patient risk stratification should follow In stable CAD, the functional impact of coronary lesions relative to their angiographic severity has a larger role than previously in determining the role of percutaneous coronary intervention (PCI) In patients with severe symptoms or clinical characteristics suggestive of high-risk coronary anatomy: Initiate guideline-directed medical therapy For noncomplex coronary disease: Consider medical therapy first; in the presence of complex coronary lesions or if the patient has many comorbidities, coronary artery bypass grafting (CABG) is preferred over PCI; however, if the patient prefers PCI, use drug-eluting stents In patients within the lower range of intermediate PTP for stable CAD (in whom good image quality can be obtained): Consider CCTA as an alternative to stress-imaging techniques (1) to exclude stable CAD and (2) after an inconclusive exercise electrocardiogram (ECG) or stress imaging test or those in whom stress testing is contraindicated On first contact in every person with chest pain: Obtain a resting echocardiogramIn patients with a clinically important left main coronary artery stenosis: If there is only 1-vessel involvement, use PCI for ostial or mid-shaft lesions but also include a heart team discussion to decide on PCI or CABG for lesions at a distal bifurcation; for multivessel involvement, use the SYNTAX (SYNergy between percutaneous coronary intervention with TAXus and cardiac surgery) score (eg, if ≤ 22, the team should discuss, but if ≥23, CABG should be chosen) New second-line anti-anginal agents include ranolazine, nicorandil, and ivabradineHowever, the following 3 studies are not recommended[1, 2] :
Coronary calcium scoring on CT imaging in asymptomatic patientsScreening for CAD with CCTA in asymptomatic patientsStenosis quantification with CCTA in patients with a high likelihood of calcificationsIn collaboration with the European Association for the Study of Diabetes (EASD), the ESC also developed guidelines on diabetes, prediabetes, and cardiovascular diseases (CVD).[1, 3] Emphasis has been placed on the following[1, 3] :
Patient-centered careLess aggressive approach to glycemic control for the elderly and patients with "long-standing diabetes with autonomic neuropathyâ€A “simplified diagnostics†algorithm in which glycosylated hemoglobin or fasting plasma glucose studies have priority in the workup, but the oral glucose-tolerance test is reserved for "cases of uncertainty†CABG as the preferred/first revascularization choice, rather than PCISigns and symptomsThe signs and symptoms of coronary artery atherosclerosis include the following:
Chest painShortness of breathWeakness, tiredness, reduced exertional capacityDizziness, palpitationsLeg swellingWeight gainDiaphoresisStable angina pectorisIntermittent claudicationMesenteric anginaTachycardia: Common in persons with acute coronary syndrome (ACS) and acute myocardial infarction (AMI)High or low blood pressureS4 gallop: A common early findingS3 gallop: An indication of reduced left ventricular functionHeart murmursTachypneaXanthelasmasLivedo reticularisSyncopeLeg edemaRalesSee Clinical Presentation for more detail.
DiagnosisLaboratory tests:
Complete blood count (CBC)Chemistry panelLipid profileThyroid function tests: To exclude thyroid disordersBlood glucose and hemoglobin A1C (HbA1C) measurement: Appropriate in patients with diabetes mellitusMyocardial fractional flow reserve (FFR)Coronary flow reserve (CFR)Lipid studiesC-reactive protein levelSerum markersImaging studies:
EchocardiographyNuclear imagingComputed tomographyElectron beam CT scanningOptical coherence tomography imagingMagnetic resonance imagingPositron emission tomographyCoronary angiographyDoppler velocity probesUltrasonographySee Workup for more detail.
ManagementThe following are used in the management of angina[4] :
NitratesBeta blockersStatinsCalcium channel blockersRanolazineOther agents used in the treatment of coronary artery stenosis or to aid in the management of stable coronary artery disease after intervention include the following:
Angiotensin-converting enzyme inhibitors to reduce blood pressureAntiplatelet agents for acute coronary eventsIntravenous glycoprotein IIb/IIIa inhibitorsAspirinClopidogrelTiclopidineHMG-CoA reductase inhibitors, or statins to lower LDL cholesterol levelsTreatment procedures for coronary artery atherosclerosis include the following:
Coronary artery bypass grafting (CABG)Percutaneous coronary intervention (PCI)Partial ileal bypassIn high- and intermediate-risk patients with 3-vessel disease, PCI was associated with significantly higher rates of revascularization and of major adverse cardiac and cerebrovascular events than CABG[5, 6] ; the 2 procedures were equally effective in the treatment of low-risk patients with 3-vessel disease and in low- and intermediate-risk patients with left main CAD.
See Treatment and Medication for more detail.
Image library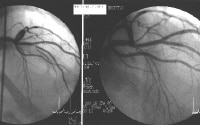 Cardiac catheterization and coronary angiography in the left panel shows severe left anterior descending coronary artery stenosis. This lesion was treated with stent placement in the left anterior descending coronary artery, as observed in the right panel. NextBackground
Cardiac catheterization and coronary angiography in the left panel shows severe left anterior descending coronary artery stenosis. This lesion was treated with stent placement in the left anterior descending coronary artery, as observed in the right panel. NextBackgroundCoronary artery atherosclerosis is the single largest killer of men and women in the United States. It is the principal cause of coronary artery disease (CAD), in which atherosclerotic changes are present within the walls of the coronary arteries. CAD is a progressive disease process that generally begins in childhood and manifests clinically in middle to late adulthood.
The word atherosclerosis is of Greek origin and literally means focal accumulation of lipid (ie, athere [gruel]) and thickening of arterial intima (ie, sclerosis [hardening]). Atherosclerosis is a disease of large and medium-sized muscular arteries and is characterized by the following:
Endothelial dysfunctionVascular inflammationBuildup of lipids, cholesterol, calcium, and cellular debris within the intima of the vessel wallAtherosclerotic buildup results in the following:
Plaque formationVascular remodelingAcute and chronic luminal obstructionAbnormalities of blood flowDiminished oxygen supply to target organsBy impairing or obstructing normal blood flow, atherosclerotic buildup causes myocardial ischemia. (See Pathophysiology.)
Approximately 14 million Americans have CAD. Each year, 1.5 million individuals develop acute myocardial infarction (AMI), the most deadly presentation of CAD, and more than 500,000 of these individuals die. (See Epidemiology.)
Nonetheless, there has been a 30% reduction in mortality from CAD since the late 20th century. Many factors have contributed to this, including the introduction of coronary care units, coronary artery bypass grafting (CABG), thrombolytic therapy, percutaneous coronary intervention (PCI), and a renewed emphasis on lifestyle modification. (See Treatment Strategies and Management.)
A major advance in the treatment of coronary artery atherosclerosis has been the development of a refined understanding of the nature of atherosclerotic plaque and the phenomenon of plaque rupture, which is the predominant cause of acute coronary syndrome (ACS) and AMI. Cardiologists now know that in many cases (perhaps more than half), the plaque that ruptures and results in the clinical syndromes of ACS and AMI is less than 50% occlusive. These so-called vulnerable plaques, as compared with stable plaques, consist of a large lipid core, inflammatory cells, and thin, fibrous caps that are subjected to greater biomechanical stress, thus leading to rupture that perpetuates thrombosis and ACS. The process of plaque rupture is illustrated in the diagram below.
 A vulnerable plaque and the mechanism of plaque rupture.
A vulnerable plaque and the mechanism of plaque rupture. The treatment of such ruptured plaques has taken a leap forward with the widespread use of newer antiplatelet and antithrombotic agents. Nonetheless, the greatest impact on the CAD epidemic can only be achieved through therapies tailored to prevent the rupture of these vulnerable plaques. Such plaques are likely more prevalent than occlusive plaques are. Currently, it is not possible to clinically identify most vulnerable plaques, and no data support the local treatment of them. On the other hand, strong evidence from many randomized trials supports the efficacy of statin-class drugs in lipid lowering and of angiotensin-converting enzyme (ACE) inhibitors in improving endothelial function, with the use of both types of agents likely leading to plaque stabilization. (See Medication.)
PreviousNextAnatomyThe healthy epicardial coronary artery consists of the following 3 layers:
IntimaMediaAdventitiaThe intima is an inner monolayer of endothelial cells lining the lumen; it is bound on the outside by internal elastic lamina, a fenestrated sheet of elastin fibers. The thin subendothelial space in between contains thin elastin and collagen fibers along with a few smooth muscle cells (SMCs).
The media are bound on the outside by an external elastic lamina that separates them from the adventitia, which consists mainly of fibroblasts, SMCs, and a matrix containing collagen and proteoglycans.
The endothelium is the monolayered inner lining of the vascular system. It covers almost 700 m2 and weighs 1.5 kg.
The endothelium has various functions. It provides a nonthrombogenic surface via a surface covering of heparan sulfate and through the production of prostaglandin derivatives such as prostacyclin, which is a potent vasodilator and an inhibitor of platelet aggregation.
The endothelium secretes the most potent vasodilator, endothelium-derived relaxing factor (EDRF), a thiolated form of nitric oxide. EDRF formation by endothelium is critical in maintaining a balance between vasoconstriction and vasodilation in the process of arterial homeostasis. The endothelium also secretes agents that are effective in lysing fibrin clots. These agents include plasminogen and procoagulant materials, such as von Willebrand factor and type 1 plasminogen activator inhibitor. In addition, the endothelium secretes various cytokines and adhesion molecules, such as vascular cell adhesion molecule-1 and intercellular adhesion molecule-1, and numerous vasoactive agents, such as endothelin, A-II, serotonin, and platelet-derived growth factor, which may be important in vasoconstriction.
Endothelium, through the above mechanisms, regulates the following:
Vascular tonePlatelet activationMonocyte adhesion and inflammationThrombus generationLipid metabolismCellular growth and vascular remodelingPreviousNextPathophysiologyInitially thought to be a chronic, slowly progressive, degenerative disease, atherosclerosis is a disorder with periods of activity and quiescence. Although a systemic disease, atherosclerosis manifests in a focal manner and affects different organ systems in different patients for reasons that remain unclear
Plaque growth and vascular remodelingThe lesions of atherosclerosis do not occur in a random fashion. Hemodynamic factors interact with the activated vascular endothelium. Fluid shear stresses generated by blood flow influence the phenotype of the endothelial cells by modulation of gene expression and regulation of the activity of flow-sensitive proteins.
Atherosclerotic plaques (or atheromas), which may require 10-15 years for full development, characteristically occur in regions of branching and marked curvature at areas of geometric irregularity and where blood undergoes sudden changes in velocity and direction of flow. Decreased shear stress and turbulence may promote atherogenesis at these important sites within the coronary arteries, the major branches of the thoracic and abdominal aorta, and the large conduit vessels of the lower extremities.
A study by Samady et al suggests low shear segments in the coronary arteries develop greater plaque and necrotic core progression and constrictive remodeling, whereas high shear segments develop greater necrotic core and calcium progression, regression of fibrous and fibrofatty tissue, and excessive expansive remodeling.[7] This suggests a transformation to a more vulnerable phenotype.
The earliest pathologic lesion of atherosclerosis is the fatty streak, which is observed in the aorta and coronary arteries of most individuals by age 20 years. The fatty streak is the result of focal accumulation of serum lipoproteins within the intima of the vessel wall. Microscopy reveals lipid-laden macrophages, T lymphocytes, and smooth muscle cells in varying proportions. The fatty streak may progress to form a fibrous plaque, the result of progressive lipid accumulation and the migration and proliferation of SMCs.
Platelet-derived growth factor, insulinlike growth factor, transforming growth factors alpha and beta, thrombin, and angiotensin II (A-II) are potent mitogens that are produced by activated platelets, macrophages, and dysfunctional endothelial cells that characterize early atherogenesis, vascular inflammation, and platelet-rich thrombosis at sites of endothelial disruption. The relative deficiency of endothelium-derived nitric oxide further potentiates this proliferative stage of plaque maturation.
The SMCs are responsible for the deposition of extracellular connective tissue matrix and form a fibrous cap that overlies a core of lipid-laden foam cells, extracellular lipid, and necrotic cellular debris. Growth of the fibrous plaque results in vascular remodeling, progressive luminal narrowing, blood-flow abnormalities, and compromised oxygen supply to the target organ. Human coronary arteries enlarge in response to plaque formation, and luminal stenosis may occur only when the plaque occupies more than 40% of the area bounded by the internal elastic lamina. Developing atherosclerotic plaques acquire their own microvascular network, the vasa vasorum, which are prone to hemorrhage and contribute to progression of atherosclerosis.[8]
As endothelial injury and inflammation progress, fibroatheromas grow and form the plaque. As the plaque grows, 2 types of remodeling, positive remodeling and negative remodeling, occur, as illustrated in the image below.
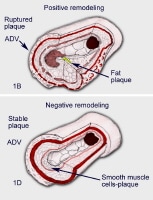 Positive and negative arterial remodeling.
Positive and negative arterial remodeling. Positive remodeling is an outward compensatory remodeling (the Glagov phenomenon) in which the arterial wall bulges outward and the lumen remains uncompromised. Such plaques grow further; however, they usually do not cause angina, because they do not become hemodynamically significant for a long time. In fact, the plaque does not begin to encroach on the lumen until it occupies 40% of the cross-sectional area. The encroachment must be at least 50-70% to cause flow limitation. Such positively remodeled lesions thus form the bulk of the vulnerable plaques, grow for years, and are more prone to result in plaque rupture and ACS than stable angina, as documented by intravascular ultrasonography (IVUS) studies.
Many fewer lesions exhibit almost no compensatory vascular dilation, and the atheroma steadily grows inward, causing gradual luminal narrowing. Many of the plaques with initial positive remodeling eventually progress to the negative remodeling stage, causing narrowing of the vascular lumen. Such plaques usually lead to the development of stable angina. They are also vulnerable to plaque rupture and thrombosis.
Plaque ruptureDenudation of the overlying endothelium or rupture of the protective fibrous cap may result in exposure of the thrombogenic contents of the core of the plaque to the circulating blood. This exposure constitutes an advanced or complicated lesion. The plaque rupture occurs due to weakening of the fibrous cap. Inflammatory cells localize to the shoulder region of the vulnerable plaque. T lymphocytes elaborate interferon gamma, an important cytokine that impairs vascular smooth muscle cell proliferation and collagen synthesis. Furthermore, activated macrophages produce matrix metalloproteinases that degrade collagen.
These mechanisms explain the predisposition to plaque rupture and highlight the role of inflammation in the genesis of the complications of the fibrous atheromatous plaque. A plaque rupture may result in thrombus formation, partial or complete occlusion of the blood vessel, and progression of the atherosclerotic lesion due to organization of the thrombus and incorporation within the plaque.
Plaque rupture is the main event that causes acute presentations. However, severely obstructive coronary atheromas do not usually cause ACS and MI. In fact, most of the atheromas that cause ACS are less than 50% occlusive, as demonstrated by coronary arteriography. Atheromas with smaller obstruction experience greater wall tension, which changes in direct proportion to their radii.
Most plaque ruptures occur because of disruption of the fibrous cap, which allows contact between the highly thrombogenic lipid core and the blood. These modestly obstructive plaques, which have a greater burden of soft lipid core and thinner fibrous caps with chemoactive cellular infiltration near the shoulder region, are called vulnerable plaques. The amount of collagen in the fibrous cap depends on the balance between synthesis and destruction of intercellular matrix and inflammatory cell activation.
T cells that accumulate at sites of plaque rupture and thrombosis produce the cytokine interferon gamma, which inhibits collagen synthesis. Already-formed collagen is degraded by macrophages that produce proteolytic enzymes and by matrix metalloproteinases (MMPs), particularly MMP-1, MMP-13, MMP-3, and MMP-9. The MMPs are induced by macrophage- and SMC-derived cytokines such as IL-1, tumor necrosis factor (TNF), and CD154 or TNF-alpha. Authorities postulate that lipid lowering stabilizes the vulnerable plaques by modulating the activity of the macrophage-derived MMPs.
Histologic composition and structureA system devised by Stary et al classifies atherosclerotic lesions according to their histologic composition and structure.[9]
In a type I lesion, the endothelium expresses surface adhesion molecules E selectin and P selectin, attracting more polymorphonuclear cells and monocytes in the subendothelial space.
In a type II lesion, macrophages begin to take up large amounts of LDL (fatty streak).
In a type III lesion, as the process continues, macrophages become foam cells.
In a type IV lesion, lipid exudes into the extracellular space and begins to coalesce to form the lipid core.
In a type V lesion, SMCs and fibroblasts move in, forming fibroatheromas with soft inner lipid cores and outer fibrous caps.
In a type VI lesion, rupture of the fibrous cap with resultant thrombosis causes ACS.
As lesions stabilize, they become fibrocalcific (type VII lesion) and, ultimately, fibrotic with extensive collagen content (type VIII lesion).
PreviousNextEtiologyA complex and incompletely understood interaction is observed between the critical cellular elements of the atherosclerotic lesion. These cellular elements include endothelial cells, smooth muscle cells, platelets, and leukocytes. Interrelated biologic processes that contribute to atherogenesis and the clinical manifestations of atherosclerosis are as follows:
Vasomotor functionThrombogenicity of the blood vessel wallState of activation of the coagulation cascadeThe fibrinolytic systemSMC migration and proliferationCellular inflammationThe encrustation theory, proposed by Rokitansky in 1851, suggested that atherosclerosis begins in the intima with deposition of thrombus and its subsequent organization by the infiltration of fibroblasts and secondary lipid deposition.
In 1856, Virchow proposed that atherosclerosis starts with lipid transudation into the arterial wall and its interaction with cellular and extracellular elements, causing "intimal proliferation."
Endothelial injury as the mechanism of atherosclerosisIn his response-to-injury hypothesis, Ross postulated that atherosclerosis begins with endothelial injury, making the endothelium susceptible to the accumulation of lipids and the deposition of thrombus. The mechanisms of atherogenesis remain uncertain, but the response-to-injury hypothesis is the most widely accepted proposal.
In the 1990s, Ross and Fuster proposed that vascular injury starts the atherosclerotic process.[10] Such injuries can be classified as follows:
Type I - Vascular injury involving functional changes in the endothelium, with minimal structural changes, (ie, increased lipoprotein permeability and white blood cell adhesion) Type II - Vascular injury involving endothelial disruption, with minimal thrombosisType III - Vascular injury involving damage to media, which may stimulate severe thrombosis, resulting in unstable coronary syndromesAccording to the response-to–vascular injury theory, injury to the endothelium by local disturbances of blood flow at angulated or branch points, along with systemic risk factors, perpetuates a series of events that culminate in the development of atherosclerotic plaque.
As discussed in greater detail below, endothelial damage occurs in many clinical settings and can be demonstrated in individuals with dyslipidemia, hypertension, diabetes, advanced age, nicotine exposure, and products of infective organisms (ie, Chlamydia pneumoniae). Damage to the endothelium may cause changes that are localized or generalized and that are transient or persistent, as follows:
Increased permeability to lipoproteinsDecreased nitric oxide productionIncreased leukocyte migration and adhesionProthrombotic dominanceVascular growth stimulationVasoactive substance releaseEndothelial dysfunction is the initial step that allows diffusion of lipids and inflammatory cells (ie, monocytes, T lymphocytes) into the endothelial and subendothelial spaces. Secretion of cytokines and growth factors promotes intimal migration, SMC proliferation, and accumulation of collagen matrix and of monocytes and other white blood cells, forming an atheroma. More advanced atheromas, even though nonocclusive, may rupture, thus leading to thrombosis and the development of ACS and MI.
Role of low-density lipoprotein-oxidative stressThe most atherogenic type of lipid is the low-density lipoprotein (LDL) component of total serum cholesterol. The endothelium's ability to modify lipoproteins may be particularly important in atherogenesis. LDLs appear to be modified by a process of low-level oxidation when bound to the LDL receptor, internalized, and transported through the endothelium. LDLs initially accrue in the subendothelial space and stimulate vascular cells to produce cytokines for recruiting monocytes, which causes further LDL oxidation. Extensively oxidized LDL (oxLDL), which is exceedingly atherogenic, is picked up by the scavenger receptors on macrophages, which absorb the LDL.
Cholesterol accumulation in macrophages is promoted by oxLDL; the macrophages then become foam cells. In addition, oxLDL enhances endothelial production of leukocyte adhesion molecules (ie, cytokines and growth factors that regulate SMC proliferation, collagen degradation, and thrombosis [eg, vascular cell adhesion molecule-1, intercellular cell adhesion molecule-1]).
Oxidized LDL inhibits nitric oxide synthase activity and increasing reactive oxygen species generation (eg, superoxide, hydrogen peroxide), thus reducing endothelium-dependent vasodilation. Moreover, oxLDL alters the SMC response to A-II stimulation and increasing vascular A-II concentrations. The SMCs that proliferate in the intima to form advanced atheromas are originally derived from the media. The theory that accumulation of SMCs in the intima represents the sine qua non of the lesions of advanced atherosclerosis is now widely accepted.
Substantial evidence suggests that oxLDL is the prominent component of atheromas. Antibodies against oxLDL react with atherosclerotic plaques, and plasma levels of immunoreactive altered LDL are greater in persons with AMI than in controls. Oxidative stress has therefore been recognized as the most significant contributor to atherosclerosis by causing LDL oxidation and increasing nitric oxide breakdown.
Risk factors for coronary artery atherosclerosisA number of large epidemiologic studies in North America and Europe have identified numerous risk factors for the development and progression of atherosclerosis. These factors, which can be classified as either modifiable or nonmodifiable, include the following:
Hyperlipidemia and dyslipidemiaHypertensionCigarette habituationAir pollutionDiabetes mellitusAgeSexThe American College of Cardiology Foundation/American Heart Association 2010 report on cardiovascular risk assessment in asymptomatic adults recommends global risk scoring (eg, Framingham Risk Score[11] ) and a family history of cardiovascular disease be obtained in all adult women and men.[12]
Numerous novel risk factors have been identified that add to the predictive value of the established risk factors and may prove to be a target for future medical interventions.
Risk factors specific to women include pregnancy and complications of pregnancy such as gestational diabetes, preeclampsia, third trimester bleeding, preterm birth, and birth of an infant small for gestational age. The 2011 update to the American Heart Association guideline for the prevention of cardiovascular disease (CVD) in women recommends that risk assessment at any stage of life include a detailed history of pregnancy complications. It also states that postpartum, obstetricians should refer women who experience these complications to a primary care physician or cardiologist.[13]
The presence of risk factors accelerates the rate of development of atherosclerosis. Diabetes causes endothelial dysfunction, decreases endothelial thromboresistance, and increases platelet activity, thus accelerating atherosclerosis.
Established risk factors successfully predict future cardiac events in about 50-60% of patients. A concerted effort to identify is also being made to validate new markers of future risk of the clinical consequences of atherosclerosis has been made.
Other risk factors for coronary artery atherosclerosis include the following:
Family history of premature CADHypoalphalipoproteinemiaObesityPhysical inactivitySyndromes of accelerated atherosclerosis - Graft atherosclerosis, CAD after cardiac transplantationChronic kidney disease[14] Systemic lupus erythematosus[15] Rheumatoid arthritis[16] Metabolic syndrome[17] Chronic inflammationInfectious agentsIncreased fibrinogen levelsIncreased lipoprotein(a) levelsFamilial hypercholesterolemiaDepressionAccording to the 2011 update to the American Heart Association guideline for CVD prevention in women, risk factors that are more common or may be more significant in women include psychosocial factors such as depression and autoimmune diseases such as systemic lupus erythematosus and rheumatoid arthritis. The Heart and Estrogen/progestin Replacement Study evaluated the effects of hormone replacement therapy on cardiovascular events among postmenopausal women with CAD and found that sudden cardiac death comprised most cardiac deaths among this group of women.[18] Women with these conditions should be evaluated for CVD and for other risk factors. Women with clinically evident CVD should also be screened for these conditions, which can affect adherence or otherwise complicate secondary CVD prevention efforts.[13]
A study by Semba et al, however, suggests that high concentrations of plasma klotho, a recently discovered hormone that has been implicated in atherosclerosis, are independently associated with a lower likelihood of having CVD.[19]
For more information, see Risk Factors for Coronary Artery Disease.
PreviousNextEpidemiologyThe true frequency of atherosclerosis is difficult, if not impossible, to accurately determine because it is a predominantly asymptomatic condition. The process of atherosclerosis begins in childhood with the development of fatty streaks. These lesions can be found in the aorta shortly after birth and appear in increasing numbers in those aged 8-18 years. More advanced lesions begin to develop when individuals are aged approximately 25 years. Subsequently, an increasing prevalence of the advanced complicated lesions of atherosclerosis is noted, and the organ-specific clinical manifestations of the disease increase with age through the fifth and sixth decades of life.
United States statisticsIn the United States, approximately 14 million persons experience CAD and its various complications. Congestive heart failure (CHF) that develops because of ischemic cardiomyopathy in hypertensive MI survivors has become the most common discharge diagnosis for patients in American hospitals. Approximately 80 million people, or 36.3% of the population, have cardiovascular disease.
Annually, approximately 1.5 million Americans have an AMI, a third of whom die. In 2009, 785,000 Americans were estimated to have suffered a first MI, and about 470,000 Americans were estimated to have had a recurrent event. An additional 195,000 "silent" heart attacks are estimated to occur each year. About every 34 seconds, an American will have an MI. CAD remains the number 1 cause of death for men and women in the United States and is responsible for approximately 20% of all US deaths. From 1995–2005, the death rate from CAD declined 34.3%, but the actual number of deaths declined only 19.4%.
International statisticsThe international incidence of ACS and AMI, especially in developed countries, is similar to that observed in the United States. Despite consumption of rich foods, inhabitants of France and the Mediterranean region appear to have a lower incidence of CAD. This phenomenon (sometimes called the French paradox) is partly explained by greater use of alcohol, with its possible HDL-raising benefit, and by consumption of the Mediterranean diet, which includes predominant use of monounsaturated fatty acids, such as olive oil or canola oil, as well as omega-3 fatty acids, which are less atherogenic. Eskimos have been found to have a lower prevalence of CAD as a result of consuming fish oils containing omega-3 fatty acids.
The Spanish cohort of the European Prospective Investigation into Cancer and Nutrition assessed the association between consumption of fried foods and risk of coronary heart disease. They found that among people living in Spain, where olive or sunflower oil is commonly used for frying, the consumption of fried foods was not associated with coronary heart disease or with all-cause mortality. This further suggests that the Mediterranean diet may help lower the risk of CAD.[20]
Findings from the World Health Organization's Monitor Trends in Cardiovascular Diseases (MONICA) project involving 21 countries showed a 4% fall in CAD death rates. Improvement in the case fatality rate accounted for only one third of the decline. However, two thirds of the decline resulted from a reduction in the number of events. These findings strongly suggest that the largest impact on decreasing the global burden of atherosclerosis will come from prevention of events.
The frequency of clinical manifestations of atherosclerosis in Great Britain, west of Scotland in particular, is especially high. The same is true of Scandinavia in general and of Finland in particular. Russia and many of the former states of the Soviet Union have recently experienced an exponential increase in the frequency of coronary heart disease that likely is the result of widespread economic hardship and social upheaval, a high prevalence of cigarette habituation, and a diet high in saturated fats.
Westernization and the rise of coronary heart diseaseThe frequency of coronary heart disease in the Far East is significantly lower than that documented in the West. Ill-defined genetic reasons for this phenomenon may exist, but significant interest surrounds the role of diet and other environmental factors in the absence of clinical atherosclerotic vascular disease in these populations. Atherosclerotic cardiovascular disease is also rare on the African continent, although growing evidence indicates that this too is changing, as a result of rapid westernization and urbanization of the traditionally rural and agrarian African populations. The prevalence of coronary heart disease is also increasing in the Middle East, India, and Central and South America.[8] The rate of CAD in ethnic immigrant populations in the United States approaches that of the disease in whites, supporting the role of these putative environmental factors.
Race-associated prevalences of coronary artery diseaseThe incidence, prevalence, and manifestations of CAD vary significantly with race, as does the response to therapy.
Blacks appear to have higher morbidity and mortality rates of CAD, even when the statistics are corrected for educational and socioeconomic status. The risk-factor burden experienced by blacks differs from that of whites. The prevalence of hypertension, obesity, dysmetabolic syndrome, and lack of physical activity are much higher in blacks, whereas the prevalence of hypercholesterolemia is lower. Blacks with AMI present for treatment later than patients do on average, are less often subjected to invasive strategies, and experience greater overall mortality. (Similar statistics can also be cited for presentation and treatment of patients with stable CAD.)
Asian Indians exhibit a 2- to 3-fold higher prevalence of CAD than do whites in the United States. They also have greater prevalences of hypoalphalipoproteinemia, high lipoprotein(a) levels, and diabetes.
Sex-associated prevalences of coronary artery diseaseMen traditionally have a higher prevalence of CAD. Women, however, follow men by 10 years, especially after menopause. (The value of estrogen supplementation for prevention of CAD has been discredited by the Heart and Estrogen/Progestin Replacement Study [HERS]).[21, 22]
The presence of diabetes, as well as tobacco use, eliminates the protection from heart disease associated with female sex. In women, as in men, the most common cause of death is CAD, which accounts for more deaths in women than those related to breast and uterine diseases combined. Women with AMI present later than average, are less often subjected to invasive strategies, and experience greater overall mortality. (Similar statistics can also be cited for the presentation and treatment of patients with stable CAD.)
The 2011 update to the American Heart Association guideline for the prevention of cardiovascular disease in women recommends changes in prevention and treatment practices:[13]
Women should be considered as high risk, and as candidates for aggressive treatment, if their risk of dying from any cardiovascular event in the next 10 years is 10% or greater. Research studies should publish efficacy and adverse drug reactions (ADRs) by gender, as both can differ in women.Evidence from clinical trials tends to overestimate the real-world efficacy of therapies in female patients, who are generally older and have more comorbidities than test subjects. The guideline is now “effectiveness-based†rather than “evidence-based.†Effectiveness-based considerations have reduced the strength of previous recommendations for use of aspirin, statins (in women with elevated C-reactive protein but normal cholesterol), and aggressive glycemic control in diabetes. The elderly and coronary artery diseaseAge is the strongest risk factor for the development of CAD. Most cases of CAD become clinically apparent in patients aged 40 years or older, but elderly persons experience higher mortality and morbidity rates from it. Approximately 82% of people who die of CAD are 65 years or older. Complication rates of multiple therapeutic interventions tend to be higher in the elderly; however, the magnitude of benefit from the same interventions is greater in this population, because these patients form a high-risk subgroup.
Calculating risk of coronary artery atherosclerosisOf note, algorithms for predicting the risk of cardiovascular disease have generally been developed for a follow-up period of no more than 10 years. However, clustering of risk factors at younger ages and increasing life expectancy suggest the need for longer-term risk prediction.
In a prospective, 30-year follow-up study, standard risk factors (male sex, systolic blood pressure, antihypertensive treatment, total and high-density lipoprotein cholesterol, smoking, diabetes mellitus), measured at baseline, were significantly related to the incidence of coronary death, myocardial infarction, and stroke and remained significant when updated regularly. This 2009 study by Pencina and colleagues, which utilized 4506 participants of the Framingham Offspring cohort, employed an algorithm for predicting 30-year risk for the above events. The investigators also found that body mass index was associated positively with 30-year risk of such events, but only in models that did not update risk factors.[11]
PreviousNextPrognosisAs previously mentioned, approximately 1.5 million Americans per year have an AMI, with a third of these events proving fatal. The survivors of MI have a poor prognosis, carrying a 1.5- to 15-fold higher risk of mortality and morbidity than the rest of the population. Historically, for example, 25% of men and 38% of women die within 1 year after having an MI, although these rates may overstate the 1-year mortality rate today, given advances in the treatment of CHF and sudden cardiac death. Among survivors, 18% of men and 34% of women have a second MI within 6 years, 7% of men and 6% of women die suddenly, 22% of men and 46% of women are disabled with CHF, and 8% of men and 11% of women have a stroke.
The prognosis in patients with atherosclerosis depends on the following factors:
Presence of inducible ischemiaLeft ventricular functionPresence of arrhythmiasRevascularization potential (complete vs incomplete)Aggressiveness of risk alterationCompliance with medical therapyThe prognosis of atherosclerosis also depends on systemic burden of disease, the vascular bed(s) involved, and the degree of flow limitation. Wide variability is noted, and clinicians appreciate that many patients with critical limitation of flow to vital organs may survive many years, despite a heavy burden of disease. Conversely, MI or sudden cardiac death may be the first clinical manifestation of atherosclerotic cardiovascular disease in a patient who is otherwise asymptomatic with minimal luminal stenosis and a light burden of disease.
Much of this phenotypic variability is likely to be determined by the relative stability of the vascular plaque burden. Plaque rupture and exposure of the thrombogenic lipid core are critical events in the expression of this disease process and determine the prognosis. The ability to determine and quantify risk and prognosis in patients with atherosclerosis is limited by the inability to objectively measure plaque stability and other predictors of clinical events.
PreviousNextPatient EducationEducation regarding CAD is extremely important. Publications and articles available from the American Heart Association provide a wealth of information.
The most effective and probably the most cost-efficient means of reducing the burden of disease secondary to atherosclerosis in the general population is primary prevention. The role of diet and exercise in the prevention of atherosclerotic cardiovascular disease has been well established. Education of the general population regarding healthy dietary habits and regular exercise will reduce the prevalence of multiple coronary heart disease risk factors. (See Treatment Strategies and Management) For patients with risk factors refractory to lifestyle interventions, education can enhance compliance with prescribed therapy.
For excellent patient education resources, visit eMedicineHealth's Cholesterol Center.
Also, see eMedicineHealth's patient education articles High Cholesterol, Lifestyle Cholesterol Management, Chest Pain, Coronary Heart Disease, Heart Attack, Angina Pectoris, and Statins for Cholesterol.
PreviousProceed to Clinical Presentation , Coronary Artery Atherosclerosis










0 comments:
Post a Comment