Cor pulmonale is defined as an alteration in the structure and function of the right ventricle caused by a primary disorder of the respiratory system. Pulmonary hypertension is the common link between lung dysfunction and the heart in cor pulmonale. Right-sided ventricular disease caused by a primary abnormality of the left side of the heart or congenital heart disease is not considered cor pulmonale, but cor pulmonale can develop secondary to a wide variety of cardiopulmonary disease processes. Although cor pulmonale commonly has a chronic and slowly progressive course, acute onset or worsening cor pulmonale with life-threatening complications can occur.[1]
NextEtiology and Pathophysiology of Cor PulmonaleCor pulmonale usually presents chronically, but 2 main conditions can cause acute cor pulmonale: pulmonary embolism (more common) and acute respiratory distress syndrome (ARDS). The underlying pathophysiology in massive pulmonary embolism causing cor pulmonale is the sudden increase in pulmonary resistance. In ARDS, 2 factors cause right ventricular (RV) overload: the pathologic features of the syndrome itself and mechanical ventilation. Mechanical ventilation, especially higher tidal volume, requires a higher transpulmonary pressure.
In chronic cor pulmonale, RV hypertrophy (RVH) generally predominates. In acute cor pulmonale, right ventricular dilatation mainly occurs. In the case of ARDS, cor pulmonale is associated with increased possibility of right-to-left shunt through the patent foramen ovale and carries a poorer prognosis.[2]
Several different pathophysiologic mechanisms can lead to pulmonary hypertension and, subsequently, to cor pulmonale. These pathogenetic mechanisms include the following:
Pulmonary vasoconstriction due to alveolar hypoxia or blood acidemia – This can result in pulmonary hypertension and if the hypertension is severe enough, it causes cor pulmonale. Anatomic compromise of the pulmonary vascular bed secondary to parenchymal or alveolar lung disorders (eg, emphysema, pulmonary thromboembolism, interstitial lung disease, adult respiratory distress syndrome, and rheumatoid disorders) – These conditions can cause elevated pulmonary blood pressure. Chronic obstructive pulmonary disorder is the most common cause of cor pulmonale, and some connective tissue disorders with pulmonary involvement may result in pulmonary hypertension and cor pulmonale. Increased blood viscosity secondary to blood disorders (eg, polycythemia vera, sickle cell disease, macroglobulinemia)Increased blood flow in pulmonary vasculatureIdiopathic primary pulmonary hypertensionThe result of the above mechanisms is increased pulmonary arterial pressure.
RV and LV outputThe RV is a thin-walled chamber that is more a volume pump than a pressure pump. It adapts better to changing preloads than afterloads. With an increase in afterload, the RV increases systolic pressure to keep the gradient. At a point, a further increase in the degree of pulmonary arterial pressure produces significant RV dilatation, an increase in RV end-diastolic pressure, and RV circulatory collapse.
A decrease in RV output with a decrease in diastolic left ventricle (LV) volume results in decreased LV output. Because the right coronary artery, which supplies the RV free wall, originates from the aorta, decreased LV output diminishes blood pressure in the aorta and decreases right coronary blood flow. What ensues is a vicious cycle between decreases in LV and RV output.
RV and LV morphogenesisGenetic investigations have confirmed that morphogenesis of the right and left ventricle originated from different sets of progenitor cells and sites. This polymorphism could explain the differing rates of hypertrophy of the right and left ventricles.[3]
RV overloadRight ventricular overload is associated with septal displacement toward the left ventricle. Septal displacement, which is seen on echocardiography, can be another factor that decreases LV volume and output in the setting of cor pulmonale and RV enlargement.
PreviousNextEpidemiology of Cor PulmonaleAlthough the prevalence of COPD in the United States is about 15 million, the exact prevalence of cor pulmonale is difficult to determine, because it does not occur in all cases of COPD, and the physical examination and routine tests are relatively insensitive for the detection of pulmonary hypertension.
Cor pulmonale is estimated to account for 6-7% of all types of adult heart disease in the United States, with chronic obstructive pulmonary disease (COPD) due to chronic bronchitis or emphysema the causative factor in more than 50% of cases. In addition, cor pulmonale accounts for 10-30% of decompensated heart failure–related admissions in the United States.[4]
In contrast, acute cor pulmonale is usually secondary to massive pulmonary embolism. Acute massive pulmonary thromboembolism is the most common cause of acute life-threatening cor pulmonale in adults; 50,000 deaths in the United States are estimated to occur per year from pulmonary emboli and about half occur within the first hour due to acute right heart failure.
Globally, the incidence of cor pulmonale varies among different countries, depending on the prevalence of cigarette smoking, air pollution, and other risk factors for various lung diseases.
PreviousNextCor Pulmonale PresentationThe clinical manifestations of cor pulmonale are generally nonspecific. The symptoms may be subtle, especially in early stages of the disease, and they may be mistakenly attributed to the underlying pulmonary pathology.
SymptomsThe patient may complain of fatigue, tachypnea, exertional dyspnea, and cough. Anginal chest pain can also occur and may be due to right ventricular ischemia (it usually does not respond to nitrates) or pulmonary artery stretching. A variety of neurologic symptoms may be seen due to decreased cardiac output and hypoxemia.
Hemoptysis may occur because of rupture of a dilated or atherosclerotic pulmonary artery. Other conditions, such as tumors, bronchiectasis, and pulmonary infarction, should be excluded before attributing hemoptysis to pulmonary hypertension. Rarely, the patient may complain of hoarseness due to compression of the left recurrent laryngeal nerve by a dilated pulmonary artery.
In advanced stages, passive hepatic congestion secondary to severe right ventricular failure may lead to anorexia, right upper quadrant abdominal discomfort, and jaundice. In addition, syncope with exertion, which may also be seen in severe disease, reflects a relative inability to increase cardiac output during exercise with a subsequent drop in the systemic arterial pressure.
Elevated pulmonary artery pressure can lead to elevated right atrial, peripheral venous, and capillary pressure. By increasing the hydrostatic gradient, it leads to transudation of fluid and accumulation of peripheral edema. Although this is the simplest explanation for peripheral edema in cor pulmonale, other hypotheses explain this symptom, especially in a fraction of patients with chronic obstructive pulmonary disease (COPD) who do not show increase in right atrial pressure. A decrease in glomerular filtration rate (GFR) and filtration of sodium and stimulation of arginine vasopressin (which decreases free water excretion) due to hypoxemia play important pathophysiologic roles in this setting and may even have a role for peripheral edema in patients with cor pulmonale who have elevated right atrial pressure.[5]
SignsPhysical findings may reflect the underlying lung disease or pulmonary hypertension, right ventricular hypertrophy (RVH), and RV failure. An increase in chest diameter, labored respiratory efforts with retractions of the chest wall, distended neck veins with prominent a or v waves, and cyanosis may be seen.
On auscultation of the lungs, wheezes and crackles may be heard as signs of underlying lung disease. Turbulent flow through recanalized vessels in chronic thromboembolic pulmonary hypertension[6] may be heard as systolic bruits in the lungs.
Splitting of the second heart sound with accentuation of the pulmonic component can be heard in early stages. A systolic ejection murmur with sharp ejection click over the region of the pulmonary artery may be heard in advanced disease, along with a diastolic pulmonary regurgitation murmur. Other findings upon auscultation of the cardiovascular system may be third and fourth sounds of the heart and systolic murmur of tricuspid regurgitation.
RVH is characterized by a left parasternal or subxiphoid heave. Hepatojugular reflux and pulsatile liver are signs of RV failure with systemic venous congestion.
On percussion, hyperresonance of the lungs may be a sign of underlying COPD; ascites can be seen in severe disease.
Examination of the lower extremities reveals evidence of pitting edema. Edema in cor pulmonale is strongly associated with hypercapnia.[7]
PreviousNextDiagnostic ConsiderationsA general approach to diagnose cor pulmonale and to investigate its etiology starts with routine laboratory tests, chest radiography, and electrocardiography. Echocardiography gives valuable information about the disease and its etiology. Right heart catheterization is the most accurate but invasive test to confirm the diagnosis of cor pulmonale and gives important information regarding the underlying diseases.
Making a diagnosis of cor pulmonale should be followed by further investigation to determine the underlying lung pathology. Sometimes a common lung disease such as chronic obstructive pulmonary disease (COPD) is not the only lung pathology as the cause of cor pulmonale; other lung diseases may coexist. Thus, pulmonary function tests may become necessary to confirm the underlying lung disease. Ventilation/perfusion (V/Q) scanning or chest computed tomography (CT) scanning may be performed if the patient’s history and physical examination suggest pulmonary thromboembolism as the cause or if other diagnostic tests do not suggest other etiologies.
Any abnormal result in each of the above tests may need further diagnostic evaluation in that specific direction.
Imaging studies may show evidence of underlying cardiopulmonary diseases, pulmonary hypertension, or its consequence, right ventricular enlargement.
Note the importance of continuous supplemental oxygen therapy in appropriate patients, as well as the dangers of cigarette smoking while using supplemental oxygen. Elevation of carboxyhemoglobin in the blood due to smoking can significantly decrease the effect of O2 on arterial O2 content.
DifferentialsWhen diagnosing cor pulmonale, it is important to consider the possibility of thromboembolic disease and primary pulmonary hypertension as possible etiologies. In addition, also assess for the following conditions:
Atrial myxomaBlood disorders that are associated with increased blood viscosityCongestive (biventricular) heart failureConstrictive pericarditisHigh-output heart failureInfiltrative cardiomyopathiesPrimary pulmonic stenosisRight heart failure due to right ventricular infarctionRight-sided heart failure due to congenital heart diseasesVentricular septal defectPreviousNextDiagnostic TestsLaboratory investigations are directed toward defining the potential underlying etiologies as well as evaluating complications of cor pulmonale. In specific instances, appropriate laboratory studies may include the following:
Hematocrit for polycythemia, which can be a consequence of underlying lung disease but which can also increase pulmonary arterial pressure by increasing viscosity Serum alpha1-antitrypsin, if deficiency is suspectedAntinuclear antibody level for collagen vascular disease, such as sclerodermaCoagulations studies to evaluate hypercoagulability states (eg, serum levels of proteins S and C, antithrombin III, factor V Leyden, anticardiolipin antibodies, homocysteine) PreviousNextArterial Blood Gas AnalysisArterial blood gas measurements may provide important information about the level of oxygenation and type of acid-base disorder.
PreviousNextBrain Natriuretic PeptideElevated brain natriuretic peptide (BNP) level alone is not adequate to establish the presence of cor pulmonale, but it helps to diagnose cor pulmonale in conjunction with other noninvasive tests and in appropriate clinical settings. An elevated BNP level may actually be a natural mechanism to compensate for elevated pulmonary hypertension and right heart failure by promoting diuresis and natriuresis, vasodilating systemic and pulmonary vessels, and reducing circulating levels of endothelin and aldosterone.
PreviousNextChest RadiographyIn patients with chronic cor pulmonale, the chest radiograph may show enlargement of the central pulmonary arteries with oligemic peripheral lung fields. Pulmonary hypertension should be suspected when the right descending pulmonary artery is larger than 16 mm in diameter and the left pulmonary artery is larger than 18 mm in diameter. Right ventricular enlargement leads to an increase of the transverse diameter of the heart shadow to the right on the posteroanterior view and filling of the retrosternal air space on the lateral view. These findings have reduced sensitivity in the presence of kyphoscoliosis or hyperinflated lungs.
PreviousNextElectrocardiographyElectrocardiographic (ECG) abnormalities in cor pulmonale reflect the presence of right ventricular hypertrophy (RVH), RV strain, or underlying pulmonary disease (see the image below). Such ECG changes may include the following:
Right axis deviationR/S amplitude ratio in V1 greater than 1 (an increase in anteriorly directed forces may be a sign of posterior infarction)R/S amplitude ratio in V6 less than 1P-pulmonale pattern (an increase in P wave amplitude in leads 2, 3, and aVF)S1 Q3 T3 pattern and incomplete (or complete) right bundle branch block, especially if pulmonary embolism is the underlying etiologyLow-voltage QRS because of underlying COPD with hyperinflationSevere RVH may reflect as Q waves in the precordial leads that may be mistakenly interpreted as an anterior myocardial infarction (however, as electrical activity of the RV is significantly less than the left ventricle [LV], small changes in RV forces may be lost in the ECG). See the image below.
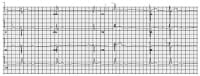 This ECG shows some typical abnormalities that may be seen in cor pulmonale and other chronic pulmonary diseases: (1) R/S ratio >1 in V1 and < 1 in V6 suggestive of right ventricular hypertrophy/enlargement, (2) right superior axis deviation, (3) left atrial type of p wave with increased width of the p wave and biphasic p wave in V1, and (4) right bundle branch block pattern with wide QRS and RsR1 pattern in V1 and slurred s wave in V6.This ECG also presents a sinus bradycardia rhythm with first-degree AV block and left anterior fascicular block.
This ECG shows some typical abnormalities that may be seen in cor pulmonale and other chronic pulmonary diseases: (1) R/S ratio >1 in V1 and < 1 in V6 suggestive of right ventricular hypertrophy/enlargement, (2) right superior axis deviation, (3) left atrial type of p wave with increased width of the p wave and biphasic p wave in V1, and (4) right bundle branch block pattern with wide QRS and RsR1 pattern in V1 and slurred s wave in V6.This ECG also presents a sinus bradycardia rhythm with first-degree AV block and left anterior fascicular block. Additionally, many rhythm disturbances may be present in chronic cor pulmonale; these range from isolated premature atrial depolarizations to various supraventricular tachycardias, including paroxysmal atrial tachycardia, multifocal atrial tachycardia, atrial fibrillation, atrial flutter, and junctional tachycardia. These dysrhythmias may be triggered by processes secondary to the underlying disease, (eg, anxiety, hypoxemia, acid-base imbalance, electrolyte disturbances, excessive use of bronchodilators, heightened sympathetic activity). Life-threatening ventricular tachyarrhythmias are less common.
In selected cases, pulmonary function testing may be indicated to determine underlying obstructive or interstitial lung disease.
PreviousNext2-D and Doppler EchocardiographyTwo-dimensional (2-D) echocardiography usually demonstrates signs of chronic right ventricular (RV) pressure overload. As this overload progresses, increased thickness of the RV wall with paradoxical motion of the interventricular septum during systole occurs. At an advanced stage, RV dilatation occurs, and the septum shows abnormal diastolic flattening. In extreme cases, the septum may actually bulge into the left ventricular (LV) cavity during diastole, resulting in decreased LV diastolic volume and reduction of LV output.
Doppler echocardiography is used to estimate pulmonary arterial pressure, taking advantage of the functional tricuspid insufficiency that is usually present in pulmonary hypertension. This imaging modality is considered the most reliable noninvasive technique to estimate pulmonary artery pressure. However, the efficacy of Doppler echocardiography may be limited by the ability to identify an adequate tricuspid regurgitant jet, which may be further enhanced by using saline contrast.[8]
PreviousNextPulmonary Thromboembolism Imaging StudiesPulmonary thromboembolism has a wide range of clinical presentations—from massive embolism with acute and severe hemodynamic instability to multiple chronic peripheral embolisms—that may present with cor pulmonale.
Ventilation/perfusion (V/Q) lung scanning, pulmonary angiography, and chest computed tomography (CT) scanning may be indicated to diagnose pulmonary thromboembolism as the underlying etiology of cor pulmonale. These studies may be performed early in the diagnostic workup if any evidence of pulmonary embolism appears in the patient’s history and physical examination. These evaluations may also be considered later in the workup if other tests are not suggestive of any other etiology.
PreviousNextUltrafast, ECG-gated CT scanningUltrafast, electrocardiographically (ECG)-gated computed tomography (CT) scanning has been evaluated to study right ventricular (RV) function. In addition to estimating RV ejection fraction (RVEF), this imaging modality can estimate RV wall mass. Although the use of ultrafast, ECG-gated CT scanning is still experimental, with further improvement, it may be used to evaluate the progression of cor pulmonale in the near future.
PreviousNextMagnetic Resonance ImagingMagnetic resonance imaging of the heart is another modality that can provide valuable information about right ventricular mass, septal flattening, and ventricular function.[9, 10]
PreviousNextNuclear ImagingRadionuclide ventriculography can noninvasively determine right ventricular ejection fraction. Myocardial perfusion may also show a permanent increase in brightness of the right ventricle.[11]
PreviousNextCardiac CatheterizationAlthough high-resolution echocardiography and magnetic resonance imaging are accurate methods to measure pulmonary pressure,[12] right heart catheterization is considered the most precise method for diagnosis and quantification of pulmonary hypertension. This procedure is indicated when echocardiography cannot assess the severity of a tricuspid regurgitant jet, thus excluding an assessment of pulmonary hypertension.
Right heart catheterization is occasionally important for differentiating cor pulmonale from occult left ventricular dysfunction, especially when the presentation is confusing. Another indication is for evaluation of the potential reversibility of pulmonary arterial hypertension with vasodilator therapy or when a left-sided heart catheterization is indicated.
PreviousNextLung BiopsyLung biopsy may occasionally be indicated to determine the etiology of underlying lung disease.
PreviousNextOverview of Cor Pulmonale ManagementMedical therapy for chronic cor pulmonale is generally focused on treatment of the underlying pulmonary disease and improving oxygenation and right ventricular (RV) function by increasing RV contractility and decreasing pulmonary vasoconstriction.[13] However, the approach might be different to some degree in an acute setting, with priority given to stabilizing the patient.
Cardiopulmonary support for patients experiencing acute cor pulmonale with resultant acute RV failure includes fluid loading and vasoconstrictor (eg, epinephrine) administration to maintain adequate blood pressure. Of course, the primary problem should be corrected, if possible. For example, for massive pulmonary embolism, consider administration of anticoagulation, thrombolytic agents or surgical embolectomy, especially if circulatory collapse is impending; consider bronchodilation and infection treatment in patients with chronic obstructive pulmonary disease (COPD); and consider steroid and immunosuppressive agents in infiltrative and fibrotic lung diseases.
Oxygen therapy, diuretics, vasodilators, digitalis, theophylline, and anticoagulation therapy are all different modalities used in the long-term management of chronic cor pulmonale.
Patient educationPatient education regarding the importance of adherence to medical therapy is vital, because appropriate treatment of both hypoxia and underlying medical illness can improve mortality and morbidity.
ComplicationsComplications of cor pulmonale include syncope, hypoxia, pedal edema, passive hepatic congestion, and death.
PreviousNextOxygen TherapyOxygen therapy is of great importance in patients with underlying chronic obstructive pulmonary disease (COPD),[14] particularly when administered on a continuous basis. With cor pulmonale, the partial pressure of oxygen (PaO2) is likely to be below 55 mm Hg and decreases further with exercise and during sleep.
Oxygen therapy relieves hypoxemic pulmonary vasoconstriction, which then improves cardiac output, lessens sympathetic vasoconstriction, alleviates tissue hypoxemia, and improves renal perfusion. The multicenter, randomized Nocturnal Oxygen Therapy Trial (NOTT) showed that continuous low-flow oxygen therapy for patients with severe COPD resulted in significant reduction in the mortality rate.[15]
In general, in patients with COPD, long-term oxygen therapy is recommended when the PaO2 is less than 55 mm Hg or the O2 saturation is less than 88%. However, in the presence of cor pulmonale or impaired mental or cognitive function, long-term oxygen therapy can be considered even if the PaO2 is greater than 55 mm Hg or the O2 saturation is greater than 88%.
Although whether oxygen therapy improves survival in patients with cor pulmonale due to pulmonary disorders other than COPD is not clear, it may provide some degree of symptomatic relief and improvement in functional status. Therefore, oxygen therapy plays an important role in both the immediate setting and long-term management, especially in patients who are hypoxic and have COPD.
PreviousNextPharmacotherapyDiuretics are used to decrease the elevated right ventricular (RV) filling volume in patients with chronic cor pulmonale. Calcium channel blockers are pulmonary artery vasodilators that have proven efficacy in the long-term management of chronic cor pulmonale secondary to primary pulmonary arterial hypertension (PAH).[16]
US Food and Drug Administration (FDA)–approved prostacyclin analogues and endothelin-receptor antagonists are available for treatment of primary pulmonary hypertension (PPH). The beneficial role of cardiac glycosides, namely digitalis, on the failing right ventricle are somewhat controversial; these agents can improve RV function but must be used with caution and should be avoided during acute episodes of hypoxia.
The main indication for oral anticoagulants in the management of cor pulmonale is in the setting of an underlying thromboembolic event or primary PAH.
Methylxanthines, like theophylline, can be used as an adjunctive treatment for chronic cor pulmonale secondary to chronic obstructive pulmonary disease (COPD). Besides the moderate bronchodilatory effect of methylxanthine, this agent improves myocardial contractility, causes a mild pulmonary vasodilatory effect, and enhances diaphragmatic contractility.
Diuretic agentsDiuretics are used in the management of chronic cor pulmonale, particularly when the RV filling volume is markedly elevated and in the management of associated peripheral edema. These agents may result in improvement of the function of both the right and left ventricles; however, diuretics may produce hemodynamic adverse effects if they are not used cautiously. Excessive volume depletion can lead to a decline in cardiac output.
Another potential complication of diuresis is the production of a hypokalemic metabolic alkalosis, which diminishes the effectiveness of carbon dioxide stimulation on the respiratory centers and lessens ventilatory drive. The adverse electrolyte and acid-base effect of diuretic use can also lead to cardiac arrhythmia, which can diminish cardiac output. Therefore, diuresis, while recommended in the management of chronic cor pulmonale, needs to be used with great caution.
Vasodilator drugsVasodilators have been advocated in the long-term management of chronic cor pulmonale with modest results. Calcium channel blockers, particularly oral sustained-release nifedipine[17] and diltiazem, can lower pulmonary pressures, although these agents appear more effective in primary rather than secondary pulmonary hypertension.[18]
Other classes of vasodilators, such as beta agonists, nitrates, and angiotensin-converting enzyme (ACE) inhibitors have been tried but, in general, vasodilators have failed to show sustained benefit in patients with COPD, and they are not routinely used. A trial of vasodilator therapy may be considered only in patients with COPD with disproportionately high pulmonary blood pressure.
Beta-selective agonist drugsBeta-selective agonists have an additional advantage of bronchodilator and mucociliary clearance effect. Right heart catheterization has been recommended during initial administration of vasodilators to objectively assess the efficacy and detect the possible adverse hemodynamic consequences of vasodilators.
The FDA approved epoprostenol, treprostinil, bosentan, and iloprost for the treatment of PPH. Epoprostenol, treprostinil, and iloprost are prostacyclin (PGI2) analogues and have potent vasodilatory properties.[19] Epoprostenol and treprostinil are administered intravenously (IV) and iloprost is an inhaler. Bosentan is a mixed endothelin-A and endothelin-B receptor antagonist indicated for PAH, including PPH. In clinical trials, bosentan improved exercise capacity, decreased rate of clinical deterioration, and improved hemodynamics.[19]
The PDE5 inhibitor sildenafil has been intensively studied[20, 21, 22] and was approved by the FDA for treatment of pulmonary hypertension. Sildenafil promotes selective smooth muscle relaxation in lung vasculature.[23] Tadalafil, another PDE5 inhibitor, was also approved by the FDA for the treatment of PAH to improve exercise ability.[24]
There are not enough data available yet regarding the efficacy of these drugs in patients with secondary pulmonary hypertension, such as in patients with COPD.
Cardiac glycoside agentsThe use of cardiac glycosides, such as digitalis, in patients with cor pulmonale has been controversial, and the beneficial effect of these drugs is not as obvious as in the setting of left heart failure. Nevertheless, studies have confirmed a modest effect of digitalis on the failing right ventricle in patients with chronic cor pulmonale.[25] This drug must be used cautiously, however, and should not be used during the acute phases of respiratory insufficiency when large fluctuations in levels of hypoxia and acidosis may occur. Patients with hypoxemia or acidosis are at increased risk of developing arrhythmias due to digitalis through different mechanisms, including sympathoadrenal stimulation.
TheophyllineIn addition to bronchodilatory effects, theophylline has been reported to reduce pulmonary vascular resistance and pulmonary arterial pressures acutely in patients with chronic cor pulmonale secondary to COPD.[26] Theophylline has a weak inotropic effect and thus may improve right and left ventricular ejection. Low doses of theophylline have also been suggested to have anti-inflammatory effects that help to control underlying lung diseases such as COPD.[27] As a result, considering the use of theophylline as adjunctive therapy in the management of chronic or decompensated cor pulmonale is reasonable in patients with underlying COPD.
WarfarinAnticoagulation with warfarin is recommended in patients at high risk for thromboembolism. The beneficial role of anticoagulation in improving the symptoms and mortality in patients with primary PAH has been demonstrated in several studies.[28, 29, 30] The evidence of benefit, however, has not been established in patients with secondary PAH. Therefore, anticoagulation therapy may be used in patients with cor pulmonale secondary to thromboembolic phenomena and with underlying primary PAH.
PreviousNextSurgical Management of Cor PulmonalePhlebotomy is indicated in patients with chronic cor pulmonale and chronic hypoxia causing severe polycythemia, defined as hematocrit of 65% or more. Phlebotomy results in a decrease in mean pulmonary artery pressure, a decrease in mean pulmonary vascular resistance,[31] and an improvement in exercise performance in such patients. However, no evidence suggests improvement in survival.
Generally, phlebotomy should be reserved as an adjunctive therapy for patients with acute decompensation of cor pulmonale and patients who remain significantly polycythemic despite appropriate long-term oxygen therapy. Replacement of the acute volume loss with a saline infusion may be necessary to avoid important decreases in systemic blood pressure.
No surgical treatment exists for most diseases that cause chronic cor pulmonale. Pulmonary embolectomy is efficacious for unresolved pulmonary emboli, which contribute to pulmonary hypertension. Uvulopalatopharyngoplasty (UPPP) in selected patients with sleep apnea and hypoventilation may relieve cor pulmonale.[32]
Single-lung, double-lung, and heart-lung transplantation are all used to salvage the terminal phases of several diseases (eg, PPH, emphysema, idiopathic pulmonary fibrosis, cystic fibrosis) complicated by cor pulmonale. Lung transplantation may lead to a reversal of right ventricular dysfunction from the chronic stress of pulmonary hypertension. However, strict selection criteria for lung transplant recipients must be met because of the limited availability of organ donors.
PreviousNextOutpatient MonitoringPatients with cor pulmonale generally require close attention in the outpatient setting. It is appropriate to regularly assess the patient’s oxygen needs and pulmonary function. Consider a formal program of pulmonary rehabilitation, as many patients benefit from this therapy.
PreviousNextPrognosis of Cor PulmonaleThe prognosis of cor pulmonale is variable depending upon the underlying pathology. Development of cor pulmonale as a result of a primary pulmonary disease usually heralds a poorer prognosis. For example, patients with chronic obstructive pulmonary disease (COPD) who develop cor pulmonale have a 30% chance of surviving 5 years. However, whether cor pulmonale carries an independent prognostic value or is simply reflecting the severity of underlying COPD or other pulmonary disease is not clear.
Prognosis in the acute setting due to massive pulmonary embolism or acute respiratory distress syndrome (ARDS) has not previously been shown to be dependent on the presence or absence of cor pulmonale. However, a prospective, multicenter cohort study by Volschan et al indicated that in cases of pulmonary embolism, cor pulmonale may be a predictor of inhospital mortality.[33] The authors collected demographic, comorbidity, and clinical manifestation data on 582 patients admitted to emergency or intensive care units and diagnosed with pulmonary embolism. Assessing the information using logistic regression analysis, the investigators built a prediction model. Their results indicated that in hemodynamically stable patients with pulmonary embolism, the following factors may be independent predictors of inhospital mortality[33] :
Age older than 65 yearsBed rest for longer than 72 hoursChronic cor pulmonaleSinus tachycardiaTachypneaPrevious, Cor Pulmonale












0 comments:
Post a Comment