First reported in 1868,[1] cor triatriatum, that is, a heart with 3 atria (triatrial heart), is a congenital anomaly in which the left atrium (cor triatriatum sinistrum) or right atrium (cor triatriatum dextrum) is divided into 2 compartments by a fold of tissue, a membrane, or a fibromuscular band.[2, 3, 4, 5, 6, 7] Classically, the proximal (upper or superior) portion of the corresponding atrium receives venous blood, whereas the distal (lower or inferior) portion is in contact with the atrioventricular valve and contains the atrial appendage and the true atrial septum that bears the fossa ovalis. The membrane that separates the atrium into 2 parts varies significantly in size and shape. It may appear similar to a diaphragm or be funnel-shaped, bandlike, entirely intact (imperforate) or contain 1 or more openings (fenestrations) ranging from small, restrictive-type to large and widely open. See the images below.
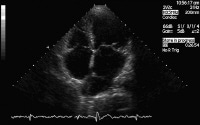 Cor triatriatum. Echocardiogram showing the proximal chamber (PC) and distal chamber (DC) of the left atrium; the right atrium (RA), left ventricle (LV), and right ventricle (RV) also are shown. Image courtesy of Guido Giordano, MD, Cardiovascular Department, Azienda Ospedaliera Cannizzaro, Catania, Italy.
Cor triatriatum. Echocardiogram showing the proximal chamber (PC) and distal chamber (DC) of the left atrium; the right atrium (RA), left ventricle (LV), and right ventricle (RV) also are shown. Image courtesy of Guido Giordano, MD, Cardiovascular Department, Azienda Ospedaliera Cannizzaro, Catania, Italy.  Cor triatriatum. Image courtesy of Guido Giordano, MD, Cardiovascular Department, Azienda Ospedaliera Cannizzaro, Catania, Italy.
Cor triatriatum. Image courtesy of Guido Giordano, MD, Cardiovascular Department, Azienda Ospedaliera Cannizzaro, Catania, Italy.  Cor triatriatum. Image courtesy of Guido Giordano, MD, Cardiovascular Department, Azienda Ospedaliera Cannizzaro, Catania, Italy.
Cor triatriatum. Image courtesy of Guido Giordano, MD, Cardiovascular Department, Azienda Ospedaliera Cannizzaro, Catania, Italy. In the pediatric population, this anomaly may be associated with major congenital cardiac lesions such as tetralogy of Fallot, double outlet right ventricle, coarctation of the aorta, partial anomalous pulmonary venous connection, persistent left superior vena cava with unroofed coronary sinus, ventricular septal defect, atrioventricular septal (endocardial cushion) defect, and common atrioventricular canal.[8, 9, 10] Rarely, asplenia or polysplenia has been reported in these patients. Although frequently an isolated finding,[11, 12, 13, 14, 15, 16, 17, 18] cor triatriatum in the adult has been reported in association with ostium secundum atrial septal defect, dilated coronary sinus due to persistent left superior vena cava, and bicuspid aortic valve.[19]
Cor triatriatum dextrum is extremely rare and results from the complete persistence of the right sinus valve of the embryonic heart. The membrane divides the right atrium into a proximal (upper) and a distal (lower) chamber. The upper chamber receives the venous blood from both vena cavae and the lower chamber is in contact with the tricuspid valve and the right atrial appendage.
NextPathophysiologyCor triatriatum sinistrumThe most popular theory holds that cor triatriatum sinister occurs when the common pulmonary vein fails to incorporate the pulmonary circulation into the left atrium and the common pulmonary venous ostium remains narrow (malincorporation theory). The result is a septum-like structure that divides the left atrium into 2 compartments. However, this theory fails to explain the presence of fossa ovalis and atrial muscle fibers within the walls of the proximal chamber where only a venous wall is supposed to be present.[20, 21, 22, 23, 24, 25, 26, 27, 28]
In addition, several cases have been reported in which 1 or 2 pulmonary veins drain into the proximal (accessory) chamber and the others drain directly into the true left atrium. Others believe that the membrane dividing the left atrium is an abnormal growth of the septum primum (malseptation theory) or that the right horn of the embryonic sinus venosus entraps the common pulmonary vein and thereby prevents its incorporation into the left atrium (entrapment theory). The significance of a prominent or persistent left superior vena cava in the pathogenesis of cor triatriatum is unclear.
Cor triatriatum dextrumDuring embryogenesis, the right horn of the sinus venosus gradually incorporates into the right atrium to form the smooth posterior portion of the right atrium, whereas the original embryologic right atrium forms the trabeculated anterior portion. The right horn of the sinus venosus and the embryologic right atrium are then connected through the sinoatrial orifice, which has on either side the 2 valvular folds called the right and left venous valves. During this incorporation, the right valve of the right horn of the sinus venosus divides the right atrium in 2. This right valve forms a sheet that serves to direct the oxygenated venous return from the inferior vena cava across the foramen ovale to the left side of the heart during fetal life (Chiari network).[29, 30, 31, 32, 33, 34, 35, 36]
Normally, this network regresses and leaves behind the crista terminalis superiorly and the eustachian valve of the inferior vena cava and the thebesian valve of the coronary sinus inferiorly. Complete persistence of the right sinus valve of embryonic life results in separation of the smooth and trabeculated portions of the right atrium and constitutes cor triatriatum dextrum. If this membrane is extensively fenestrated and weblike in appearance, then it is referred to as the Chiari network.
PreviousNextEpidemiologyFrequencyUnited StatesThe incidence of cor triatriatum has been variously reported as 0.1-0.4%.An incidence of 0.4% has been reported at autopsy of patients with congenital cardiac disease.An incidence of 0.2% was reported among patients undergoing transesophageal echocardiography.In high-volume echocardiographic laboratories, the incidence of cor triatriatum is less than 1 in 10,000. However, this is expected to rise with the increasing use of cardiac diagnostic studies.[37] Cor triatriatum dextrum is extremely rare.Cor triatriatum sinistrum can be misdiagnosed as other common cardiac or pulmonary conditions such as bronchial asthma or mitral stenosis. Mortality/MorbidityThe morbidity and mortality of cor triatriatum sinistrum is high in those who are symptomatic in infancy. This is due to the severely restrictive opening in the accessory membrane and the association with major cyanotic or acyanotic congenital heart lesions. Mortality may exceed 75% in untreated symptomatic infants. Significant sequelae is unusual with cor triatriatum dextrum as it is not commonly associated with life-threatening symptoms or major congenital cardiac defects. SexNo clear difference has been noted in incidence or clinical presentation among men or women.
AgeIn symptomatic infants, cor triatriatum sinistrum is often associated with other major congenital cardiovascular defects.In the adult, cor triatriatum sinistrum can be as follows: Asymptomatic (found incidentally on cardiac imaging)An isolated finding with a large non-restrictive communication between the superior and inferior left atrial chambersAssociated with minor congenital defects such as patent foramen ovale, atrial septal defect, or persistent left superior vena cava Cor triatriatum dextrum can be diagnosed at any age, especially if incidentally discovered. Other congenital cardiac defects, such as atrial septal defect, may be present and demand evaluation. Cor triatriatum can also be misdiagnosed as other common cardiac conditions such as constrictive pericarditis. The cross-sectional area of the fenestration within the accessory membrane likely remains unchanged with aging. Late presentation of symptomatic disease is, thus, related to the additive effects of other cardiac conditions, such as mitral regurgitation or atrial fibrillation.[38] PreviousProceed to Clinical Presentation , Cor Triatriatum











0 comments:
Post a Comment