Ventricular septal rupture (VSR) is a rare but lethal complication of myocardial infarction (MI). The event occurs 2-8 days after an infarction and often precipitates cardiogenic shock.[1] The differential diagnosis of postinfarction cardiogenic shock should exclude free ventricular wall rupture and rupture of the papillary muscles. See the image below.
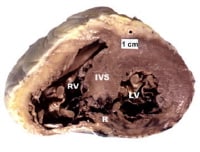 Photograph of heart sectioned transversely at level of middle left ventricle showing posterior ventricular septal defect at site of recent acute myocardial infarction.
Photograph of heart sectioned transversely at level of middle left ventricle showing posterior ventricular septal defect at site of recent acute myocardial infarction. To avoid the high morbidity and mortality associated with this disorder, patients should undergo emergency surgical treatment.[2, 3, 4, 5] In current practice, postinfarction VSR is recognized as a surgical emergency, and the presence of cardiogenic shock is an indication for intervention.[6] Long-term survival can be achieved in patients who undergo prompt surgery. Concomitant coronary artery bypass grafting (CABG) may be required. The addition of CABG has helped improve long-term survival.
Surgery is performed via a transinfarction approach, and all reconstruction is performed with prosthetic materials to avoid tension. Developments in myocardial protection and improved prosthetic materials have contributed greatly to successful management of VSR.[7] Improved surgical techniques (eg, infarctectomy) and better perioperative mechanical and pharmacologic support have helped lower mortality. In addition, the development of surgical techniques to repair perforations in different areas of the septum has led to improved results.
In current practice, patients undergoing shunt repair tend to be older and are more likely to have received thrombolytic agents, which may complicate repair. After successful repair, survival and quality of life are excellent, even in patients older than 70 years.[8]
For information, news, and CME activities on heart failure, see the Heart Failure Resource Center. For patient education resources, see the Heart Center, as well as Ventricular Septal Defect and Heart Attack.
NextPathophysiologyThe septal blood supply originates from branches of the left anterior descending coronary artery, the posterior descending branch of the right coronary artery, or the circumflex artery when it is dominant. Infarction associated with a ventricular septal rupture (VSR) is usually transmural and extensive. About 60% of VSRs occur with infarction of the anterior wall; 40% occur with infarction of the posterior or inferior wall. Posterior VSR may be accompanied by mitral valve insufficiency secondary to papillary muscle infarction or dysfunction.
At autopsy, patients with VSR usually show complete coronary artery occlusion with little or no collateral flow. The lack of collateral flow may be secondary to associated arterial disease, anatomic anomalies, or myocardial edema. Sometimes, multiple septal perforations occur. These may occur simultaneously or within several days of each other.
Ventricular aneurysms are commonly associated with postinfarction VSR and contribute significantly to the hemodynamic compromise in these patients. The reported incidence of ventricular aneurysms ranges from 35% to 68%, whereas the incidence of ventricular aneurysms alone after myocardial infarction (MI) without VSR is considerably lower (12.4%).
The natural history of postinfarction VSR is greatly influenced by hypertension, anticoagulation therapy, advanced age, and, possibly, thrombolytic therapy. The natural course in patients with postinfarction VSR is well documented and short. Most patients die within the first week, and almost 90% die within the first year; some reports indicate that fewer than 7% of patients are alive after 1 year.
This grim prognosis results from an acute volume overload exacted on both ventricles in a heart already compromised by a large MI and occasionally by extensive coronary artery disease (CAD) in sites other than that already infarcted. In addition, superimposed ischemic mitral valve regurgitation, a ventricular aneurysm, or a combination of these conditions may be present, further compromising heart function. The depressed left ventricular function commonly leads to impaired peripheral organ perfusion and death in most patients.
A few sporadic reports indicate that some patients with medically treated postinfarction VSR live for several years. Although many medical advances have been made in the nonsurgical treatment of these patients, including intra-aortic balloon counterpulsation (IABCP), these methods have not eliminated the need for surgery.
PreviousNextEpidemiologyRupture of the interventricular septum is an uncommon complication of myocardial infarction (MI). Although autopsy studies reveal an 11% incidence of myocardial free-wall rupture after MI, septal wall perforation is much less common, occurring at a rate of approximately 1-2%.
Ventricular septal rupture (VSR) occurs in a zone of necrotic myocardial tissue, usually within the first 10-14 days. Clinical studies report an average time of 2.6 days from MI to VSR. However, some data suggest that initial treatment of MI with thrombolytics may affect both the time between infarction and VSR and the eventual outcome. Early use of thrombolytic agents may lead to reopening of the occluded vessels, thereby reducing the incidence of VSR.
The age range of patients who sustain a postinfarction VSR is wide, from 44-81 years. Men are affected more commonly than women, though VSR is more common in women than would be predicted on the basis of the prevalence of coronary artery disease (CAD) alone.
PreviousNextPrognosisOperative mortality is directly related to the interval between myocardial infarction (MI) and surgical repair. If repair is performed 3 weeks or more after an infarction, mortality is approximately 20%; if it is performed before this time, mortality approaches 50%. The most obvious reason for this is that the greater the degree of myocardial damage and hemodynamic compromise, the more urgent the need for early intervention.
With the use of an early operative approach, most studies show an overall of less than 25%. Mortality tends to be lower for patients with anteriorly located ventricular septal ruptures (VSRs) and lowest for patients with apical VSRs. For anterior defects, mortality ranges from 10% to 15%; for posterior defects, mortality ranges from 30% to 35%.
More than 50% of deaths occurring after surgery for postinfarction VSR are due to cardiac failure. Sudden death is rare, and intractable heart failure can also occur. Other causes of death include cerebral embolism. Most patients who survive the hospital period have good functional status, with the majority falling into New York Heart Association (NYHA) class I or II.[9]
The most important risk factors for death in the early phase are poor hemodynamics and associated right ventricular dysfunction developing before the patient comes to the operating room. The amount and distribution of myocardial necrosis and scarring are responsible for both.
Right ventricular dysfunction results from ischemic damage or frank infarction of the right ventricle and is present when stenosis occurs in the right coronary artery system. The higher mortality observed after repair of defects located inferiorly in the septum is probably related to the higher prevalence of important right coronary artery stenosis.
The severity and distribution of coronary artery disease (CAD) are also risk factors. Similarly, advanced age at operation, diabetes, and preinfarction hypertension are risk factors for death in the early phase.
Risk factors for death in patients with postinfarction VSR may be summarized as follows:
Posteriorly located septal ruptures are technically more difficult to repair and are associated with profound right ventricular dysfunction The presence of multiple organ failure is a poor prognostic factorThe presence of cardiogenic shock does not bode well for the patient’s survivalA shortened interval between infarction and surgery usually indicates that the patient is considered more ill and therefore is at greater risk for death PreviousNextClinical PresentationUpon auscultation, a loud systolic murmur is heard, usually within the first week after an acute myocardial infarction (MI). This is the most consistent physical finding of postinfarction ventricular septal rupture (VSR). Before the development of the murmur, the patient may have been stable after the acute MI. Coincident with the onset of the murmur, the patient’s clinical course undergoes a sudden deterioration, with the development of congestive heart failure (CHF) and, often, cardiogenic shock.
The typical harsh systolic murmur is audible over a large area, including the left sternal border and apical area. It sometimes radiates to the left axilla, thereby mimicking mitral regurgitation (MR). A thrill is palpable in approximately 50% of patients.
Almost 50% of patients have recurrent chest pain. The differential diagnosis includes VSR and mitral insufficiency secondary to papillary muscle rupture, papillary muscle dysfunction, or left ventricular dilatation.
Clinical features of VSR may be summarized as follows:
The rupture typically occurs 3-8 days after an MIVSR is more likely to occur in the anterior septum than in the posterior septum (60% vs 40%)The most consistent finding is a murmurIn the differential diagnosis, exclude mitral regurgitation from papillary muscle ruptureDiagnosis is confirmed with the aid of echocardiography and the presence of a left-to-right shuntCatheterization results help determine the extent of coronary artery disease (CAD)Of patients treated without surgery, 90% dieSurgical treatment must be carried out on an emergency basis, even if the patient is stable[3] All VSRs are closed with a patch and associated coronary artery bypass grafting (CABG)Operative mortality is 10-15% for anterior defects and 30-35% for posterior defectsPreviousNextWorkupImaging studiesOn plain chest radiographs, 82% of patients with postinfarction ventricular septal rupture (VSR) demonstrate left ventricular enlargement, 78% have pulmonary edema, and 64% have a pleural effusion. These findings are nonspecific and do not exclude other causes, such as a ruptured papillary muscle.
M-mode transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) have been used to help diagnose postinfarction VSR. TTE findings have been improved with the use of color-flow Doppler methods to visualize the VSR. In addition, echocardiography can help assess the presence of any mitral valve pathology.
ElectrocardiographyNo electrocardiographic (ECG) features are diagnostic of postinfarction VSR, though ECG indeed provides some useful information. Persistent ST-segment elevation associated with ventricular aneurysm is common. ECG may reveal atrioventricular block in one third of patients. ECG can also be used to help predict the anatomic location of the septal rupture.
Catheterization and pressure measurementLeft-heart catheterization with coronary angiography is recommended in all stable patients. This procedure is time-consuming and carries some degree of morbidity in already-compromised patients; accordingly, good judgment is required when this test is ordered.
An important diagnostic test for differentiating VSR from mitral valve insufficiency is catheterization of the right heart with a Swan-Ganz catheter. In the presence of a VSR, oxygen concentration between the right atrium and the pulmonary artery is stepped up. In addition, a pulmonary capillary wedge pressure tracing is beneficial for differentiating acute mitral regurgitation (MR) from VSR.
Left- and right-side pressure measurements help estimate the degree of biventricular failure and are useful in monitoring the response to perioperative therapy. Whereas right-side failure is more common in patients with postinfarction VSR, left-side failure and refractory pulmonary edema are more prominent in patients with a ruptured papillary muscle. However, one third of patients with postinfarction VSR also have some degree of MR secondary to left ventricular dysfunction. Only rarely is VSR also associated with ruptured papillary muscle.
PreviousNextTreatment & ManagementMedical therapyInitiate pharmacologic therapy in an attempt to render the patient hemodynamically stable. The goals are to reduce afterload on the heart and to increase forward cardiac output.
Vasodilators may be used in an attempt to decrease the left-to-right shunt associated with the mechanical defect and thereby increase cardiac output. Intravenous (IV) nitroglycerin can be used as a vasodilator and may provide improved myocardial blood flow in patients with significant ischemic cardiac disease.
When used alone, inotropic agents may increase cardiac output; however, without changes in the ratio of pulmonary to systemic flow (Qp-to-Qs ratio), they markedly increase left ventricular work and myocardial oxygen consumption. The profound level of cardiogenic shock in some patients precludes vasodilator treatment, often necessitating vasopressor support.
Vasopressors markedly increase left ventricular work and myocardial oxygen consumption. They also increase systemic afterload and further increase the Qp-to-Qs ratio, thus lowering cardiac output and greatly augmenting myocardial oxygen consumption.
Intra-aortic balloon counterpulsation (IABCP) offers the most important means of temporary hemodynamic support. IABCP reduces left ventricular afterload, thus increasing systemic cardiac output and decreasing the Qp-to-Qs ratio. IABCP also facilitates diastolic augmentation with an increase in coronary blood flow, resulting in an improved oxygen supply.
IABCP is not a substitute for urgent intervention, and in patients with cardiogenic shock, it should be followed by immediate intervention. Patients with ventricular septal rupture (VSR) do not die of cardiac failure; they die as a result of end-organ failure. Only by shortening the duration of shock can the high risk of mortality be prevented.
Achieving hemodynamic stability before surgery is very beneficial, but prolonged attempts to improve the patient’s hemodynamic status can be hazardous.[10]
This aggressive approach often results in temporary stability of these extremely ill patients. As a rule, however, these benefits are brief, and patients may deteriorate rapidly. Therefore, early diagnosis and rapid surgical intervention should be planned. Only about 10-15% of patients can be treated with conservative measures for a period of 2-4 weeks, after which surgical treatment can be provided at a greatly reduced risk.
Operative therapyIndications and contraindications
In view of the grim prognosis for medically treated patients, the diagnosis of postinfarction ventricular septal rupture (VSR), by itself, constitutes an indication for operation. The controversy that once surrounded the timing of surgical intervention is no longer an issue, and most surgeons now agree that early surgery is indicated to minimize the risk of mortality and morbidity. The success of surgical therapy depends on prompt medical stabilization of the patient and prevention of cardiogenic shock.
The relative safety of repair 2-3 weeks or more after perforation has been established. Because the edges of the defect have become firmer and fibrotic, repair is more secure and is easily accomplished. A successful clinical outcome is related to the adequacy of the closure of the VSR; therefore, if possible, search for multiple defects both preoperatively and at the time of surgery.
Only when the patient is hemodynamically stable should repair be initially delayed, but there must be a high degree of certainty that the patient is in fact stable. These patients can suddenly deteriorate and die. The criteria for a delay in surgical treatment include the following:
Adequate cardiac outputNo evidence of cardiogenic shockAbsence of signs and symptoms of congestive heart failure (CHF) or minimal use of pressor agents to control initial symptomsAbsence of fluid retentionGood renal functionThe natural history of the disease is such that few patients present with these signs and symptoms. In most patients, postinfarction VSR rapidly leads to a worsening of the hemodynamic state, with cardiogenic shock, marked and intractable symptoms of CHF, and fluid retention. Immediate surgery is usually indicated.[6] The high surgical risk of early repair is accepted because of the even higher risk of death without surgery under such circumstances.
Occasionally, a delay in diagnosis and referral occurs. These patients are usually critically ill, and the prognosis is very grim; thus, allowing the natural history of the disease to take its course is prudent.[6]
Although most patients who experience postinfarction VSR need emergency surgery, an occasional patient, because a delay in either diagnosis or referral, may be in a state of multiorgan failure and may not be a candidate for surgery. The chances of such a patient surviving an operation are minimal; in these circumstances, supportive medical therapy may be adequate.[6] Patients who are comatose and in cardiogenic shock have a particularly poor prognosis after surgery, and surgery is best avoided in such circumstances.
Choice of operative approach
The first operations for repair of postinfarction VSR used an approach through the right ventricle, with an incision of the right ventricular outflow tract such as was used to repair some congenital ventriculoseptal defects (VSDs). This approach proved inadequate because of limited exposure for lesions at the apex of the heart, injury to normal right ventricular muscle, interruption of coronary collateral vessels, and failure to excise the infarcted tissue.
Subsequently, a transinfarction approach was described, which incorporated infarctectomy, aneurysmectomy, and repair of the ventricular septal perforation. Several techniques have been used to close these defects. The choice of procedure is determined by the location of the defect.
Most defects are anteroapical and are closed by buttressing the defect with viable muscle from the adjacent anterior left ventricular wall. Smaller defects located high in the ventricular septum are closed with a Dacron patch.
High posterior septal or inferior defects, which are less common, are approached through the inferior portion of the heart, usually in the distribution of the posterior descending coronary branch of the right coronary artery. The incision is made in the area of maximal infarction, which is usually on the right ventricular side of the septum. A well-proven principle of repair for these defects is the use of a synthetic patch closure to prevent tension.
Additional procedures that may be considered in the treatment of postinfarction VSR include the following:
Concomitant coronary artery bypass grafting (CABG)Mitral valve replacementExcision of left ventricular aneurysmControversy surrounds the issue of whether to perform CABG in patients undergoing emergency postinfarction ventricular septal repair. Some authors have found no benefit to CABG in this setting and have concluded that cardiac catheterization in ill patients is time-consuming and poses a risk of contrast injury to the kidney. Others, however, have used a selective approach to cardiac catheterization.
In patients who probably do not have a history of angina or previous myocardial infarction (MI), cardiac catheterization is deferred. Cardiac catheterization findings help confirm and quantitate the presence of a shunt and reveal pulmonary artery pressure and resistance values. The left ventriculogram helps determine the location and number of VSDs, define left ventricular function, and assess mitral valve function. Most surgeons perform bypass in patients with VSR, with significant improvements in survival.
Occasionally, significant mitral regurgitation (MR) may be associated with acute VSR, particularly when the infarction is posterior. In such circumstances, the mitral valve must be replaced. Replacement is usually best accomplished through the left ventriculotomy incision by using interrupted, pledged mattress sutures.
When a left ventricular aneurysm is associated with postinfarction VSR, it is excised as the initial step in surgical therapy. After repair of the VSR, the aneurysm is generally repaired.
Perioperative management
Preoperative management is directed toward rapid resuscitation and stabilization of the patient and preparation for surgery. The goals are as follows:
To reduce systemic vascular resistance (thereby decreasing the left-to-right shunt)To maintain a stable cardiac output and blood pressureTo maintain coronary artery blood flowPreoperative treatment of patients with postinfarction VSR may be summarized as follows:
Transfer patients to an intensive care unit (ICU) for resuscitationPlace a Swan-Ganz catheter to assist with hemodynamic managementDecrease the systemic vascular resistance and the left-to-right shunt with vasodilatorsMaintain cardiac output and organ perfusion with inotropic agentsMaintain coronary artery blood flowUse IABCP to decrease myocardial oxygen consumption, decrease afterload, and increase coronary artery perfusionUse mechanical ventilation as requiredUse echocardiography to help determine the site of septal ruptureUse cardiac catheterization to help determine the presence of coronary artery disease (CAD)Principles associated with the evolution of techniques for the closure of postinfarction VSR may be summarized as follows:
Determine and understand the anatomy and location of the VSR and any associated coronary artery pathologyExpeditiously establish hypothermic total cardiopulmonary bypass, and pay attention to myocardial protection with cardioplegiaUse a transinfarction approach to the VSR, with the site of ventriculotomy determined by the location of the transmural infarctionInspect the papillary muscles, and concomitantly replace the mitral valve only if frank papillary muscle rupture is presentTrim the left ventricular margins back to viable muscleConservatively trim the right ventricular muscleClose the VSR without tension, using prosthetic materialButtress the suture line with Teflon pledgets.Percutaneous techniques have been used successfully to close some congenital VSDs. Technical improvements in experimental devices for closing intracardiac shunts are being made to treat postinfarction VSR or residual shunts after primary repair. A balloon catheter introduced percutaneously has been used to abolish the shunt in poor-risk patients.
Patients who require an intra-aortic balloon pump preoperatively appear to benefit from postoperative support with the device for 24-72 hours. Some of these patients demonstrate a small persistent or recurrent left-to-right shunt. Because of the large amount of prosthetic material used to repair the septal perforation, anticoagulation therapy in these patients is recommended by some surgeons for a period of 6-8 weeks.
Residual VSDs have been noted early or late after operative treatment in 10-25% of patients. These residual defects are easily diagnosed with the aid of color-flow Doppler investigations. Residual VSDs may be attributable to the reopening of a closed defect, the presence of an overlooked VSD, or the development of a new septal perforation during the early postoperative period.
Reoperation is required for closure of such residual VSDs when the Qp-to-Qs ratio is greater than 2. When the VSDs are small and asymptomatic, a conservative approach may be recommended because spontaneous closure can occur.
Percutaneous treatmentData collected by the Society of the Thoracic Surgeons National Database indicates that post infarct VSD is a lethal disorder, even with treatment. The hope is that some type of percutaneous interventional technique may be developed in future to close the ruptured VSD and lower the mortality. Isolated reports with the amplatzer septal occluder do reveal that the technique is safe for closure of small lesions.[11, 12]
Previous, Postinfarction Ventricular Septal Rupture












ReplyDeleteThanks for this great post, i find it very interesting and very well out and put together. I look forward to reading your work in the future.
Zofran birth defects lawyer
You got a really useful blog I have been here reading for about an hour. I am a newbie and your success is very much an inspiration for me.
ReplyDeleteHip Replacement CT & Hand Injury CT