Endocardial cushion defects, more commonly known as atrioventricular (AV) canal or septal defects, include a range of defects characterized by involvement of the atrial septum, the ventricular septum, and one or both of the AV valves.
These defects can be classified by several methods. A distinction generally is made between partial and complete defects. A complete AV septal defect indicates the presence of both atrial and ventricular septal defects with a common AV valve (see image below). A partial defect indicates atrial septal involvement with separate mitral and tricuspid valve orifices.
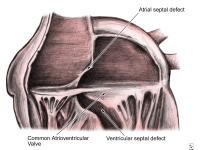 Anatomy of the endocardial cushion defect (ie, complete form); note the common atrioventricular valve straddling the atrial septal and ventricular septal defects.
Anatomy of the endocardial cushion defect (ie, complete form); note the common atrioventricular valve straddling the atrial septal and ventricular septal defects. AV canal defects arise from abnormal development of the endocardial cushions. In these patients, the superior and inferior cushions do not close completely. An interatrial communication is left at the lower portion of the atrial septum. This is called an ostium primum defect. The failure of the endocardial cushions to fuse results in an abnormally low position of the AV valves and an abnormally high position of the aortic valve. A portion of the AV valves originates from the endocardial cushions, and their improper fusion results in anterior and posterior components to the mitral valve leaflet.[1]
NextPathophysiologyPredominant left-to-right shunting of blood through the heart occurs in these patients. In patients with partial defects, this occurs through the ostium primum atrial septal defect. When a complete endocardial cushion defect is present, a large ventricular septal defect as well as valvular insufficiency may develop, resulting in volume overload of both the left and right ventricles associated with heart failure in early life. In patients with long-standing pulmonary overload, pulmonary vascular disease may develop and congestive heart failure (CHF) symptoms may improve. This improvement is a poor prognostic indicator because it heralds the development of right-to-left shunting and irreversible pulmonary hypertension (ie, Eisenmenger syndrome).[2]
PreviousNextEpidemiologyFrequencyUnited StatesThe frequency rate is about 3% of children with congenital heart disease. Sixty to seventy percent of these defects are of the complete form. More than half of those affected with the complete form have Down syndrome.
InternationalThe frequency rate is about 3% of children who have congenital heart disease.
Mortality/MorbidityPatients with only ostium primum atrial septal defect and minimal insufficiency of the left AV valve (ie, mitral valve) do well without treatment during infancy, childhood, and adolescence. During adulthood, these patients develop symptoms of CHF and atrial arrhythmia.
Patients with septal defects and mitral valve insufficiency develop CHF early in life, with high rates of morbidity and mortality if the valvular insufficiency is pronounced. Patients with a complete defect develop CHF in infancy, with frequent respiratory infections and poor weight gain.
RaceNo racial predilection is apparent.
SexGirls are affected slightly more frequently than boys.
AgeEndocardial cushion defect is a congenital defect present at birth. The severity of the symptom complex and presentation is dependent directly upon the severity of the defect and the presence of mitral insufficiency.
PreviousProceed to Clinical Presentation , Endocardial Cushion Defects












0 comments:
Post a Comment