Eisenmenger syndrome refers to any untreated congenital cardiac defect with intracardiac communication that leads to pulmonary hypertension, reversal of flow, and cyanosis.[1, 2, 3] The previous left-to-right shunt is converted into a right-to-left shunt secondary to elevated pulmonary artery pressures and associated pulmonary vascular disease. (See Etiology, Treatment, and Medication.)
Lesions in Eisenmenger syndrome, such as large septal defects, are characterized by high pulmonary pressure and/or a high pulmonary flow state. Development of the syndrome represents a point at which pulmonary hypertension is irreversible and is an indication that the cardiac lesion is likely inoperable (see the image below). (See Etiology, Workup, and Treatment.)
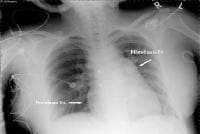 This radiograph reveals an enlarged right heart and pulmonary artery dilatation in a 24-year-old woman with an unrestricted patent ductus arteriosus (PDA) and Eisenmenger syndrome.
This radiograph reveals an enlarged right heart and pulmonary artery dilatation in a 24-year-old woman with an unrestricted patent ductus arteriosus (PDA) and Eisenmenger syndrome. Eisenmenger syndrome was initially described in 1897, when Victor Eisenmenger reported on a patient with symptoms of dyspnea and cyanosis from infancy who subsequently developed heart failure and succumbed to massive hemoptysis.[4] An autopsy revealed a large ventricular septal defect (VSD) and an overriding aorta. This was the first description of a link between a large congenital cardiac shunt defect and the development of pulmonary hypertension. (See Presentation and Workup.)
Advances in the medical treatment of patients with severe pulmonary hypertension may improve survival in patients with Eisenmenger syndrome and may potentially reverse the process in selected patients to a point at which they again become candidates for surgical repair. (See Treatment and Medication.)[5]
Pulmonary hypertensionPulmonary hypertension is defined as a mean pulmonary artery pressure of more than 25 mm Hg at rest or more than 30 mm Hg during exercise. The World Health Organization (WHO) has published a classification system of various etiologies of pulmonary hypertension; the most recent updates were in 2003 and 2008.[6, 7] Eisenmenger syndrome is considered part of the group 1 causes of pulmonary hypertension, according to the Venice classification.
Intracardiac communicationAn intracardiac communication allows high pulmonary artery pressures to develop and produces right-to-left intracardiac blood flow. Originally described in association with a large VSD, Eisenmenger syndrome can also manifest with a patent ductus arteriosus (PDA) or, less frequently, with other congenital cardiac anomalies. (See the images below.)
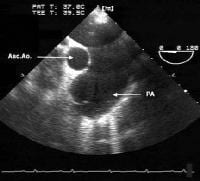 This transesophageal image is from the midesophagus of a patient with Eisenmenger syndrome secondary to an unrestricted patent ductus arteriosus (PDA). It shows a severely dilated pulmonary artery. PA = pulmonary artery, Asc Ao = ascending aorta.
This transesophageal image is from the midesophagus of a patient with Eisenmenger syndrome secondary to an unrestricted patent ductus arteriosus (PDA). It shows a severely dilated pulmonary artery. PA = pulmonary artery, Asc Ao = ascending aorta.  This computed tomography (CT) chest scan shows a large, unrestricted patent ductus arteriosus (PDA) in a 24-year-old woman with Eisenmenger syndrome.
This computed tomography (CT) chest scan shows a large, unrestricted patent ductus arteriosus (PDA) in a 24-year-old woman with Eisenmenger syndrome. Examples of congenital heart disease subtypes that may cause pulmonary vascular disease and proceed to Eisenmenger syndrome include the following:
Increased pulmonary arterial flow -Atrial septal defect (ASD), systemic arteriovenous fistulae, total anomalous pulmonary venous returnIncreased pulmonary arterial pressure and flow - Large VSD, large PDA, truncus arteriosus, single ventricle with unobstructed pulmonary blood flowElevated pulmonary venous pressure - Mitral stenosis, cor triatriatum, obstructed pulmonary venous returnNextEpidemiologyEisenmenger syndrome usually develops before puberty but may develop in adolescence and early adulthood.
Patients in underdeveloped countries are more likely to present late with uncorrected congenital cardiac lesions and a markedly elevated pulmonary vascular resistance (PVR). They are more likely to be inoperable secondary to Eisenmenger physiology.
PreviousNextEtiologyEisenmenger syndrome occurs in patients with large, congenital cardiac or surgically created extracardiac left-to-right shunts. These shunts initially cause increased pulmonary blood flow.
If left unchecked, increased pulmonary blood flow and/or elevated pulmonary arterial pressure can result in remodeling of the pulmonary microvasculature, with subsequent obstruction to pulmonary blood flow. This is commonly referred to as pulmonary vascular obstructive disease (PVOD).
According to Ohms law, flow (Q) is inversely related to resistance (R) and is directly proportional to pressure (P), as represented by the equation Q = P/R. Any increase in flow, as is observed in patients with intracardiac defects and initial left-to-right shunts, results in increased pulmonary artery pressures. Additionally, any increase in resistance, as occurs in PVOD, results in a decrease in effective flow at the same pressure.
The progression to Eisenmenger physiology is represented by a spectrum of morphologic changes in the capillary bed that progress from reversible lesions to irreversible ones. Endothelial dysfunction and smooth muscle proliferation result from the changes in flow and pressure, increasing the PVR.[8]
The cellular and molecular mechanisms remain fully uncharacterized, representing pathways of inflammation, cell proliferation, vasoconstriction, and fibrosis.[9] The mechanism of pulmonary hypertension in congenital heart disease may share characteristics with other mechanisms of pulmonary hypertension, but the pathways remain complex.
In 1958, Heath and Edwards proposed a histologic classification to describe the changes in Eisenmenger syndrome.[10] Stages I and II represent disease that is most likely reversible. Stage III disease may still be reversible, but in progressing to stages IV-VI, the disease is thought to become irreversible. Pulmonary biopsies are rarely performed today for this condition.
Natural historyFailure to reduce pulmonary pressures in the first 2 years of life may result in the failure of the normal regression of the intimal smooth muscle. This is followed by the progressive changes described by Heath and Edwards.[10] The condition then advances to irreversible pulmonary hypertension, defined as unresponsiveness to inhalation of 100% oxygen or nitric oxide. This point usually correlates to a PVR of more than 12 Woods units.
Clinically, patients gradually develop the following complications of advanced pulmonary vascular disease:
Dyspnea upon exertionSyncopeChest painStrokeBrain abscessCyanosisCongestive heart failureDysrhythmiaHyperviscosity complicationsPulmonary hemorrhage/hemoptysisEndocarditisThe timeframe for this process depends on the anatomic nature of the lesion and whether conditions, such as trisomy 21 (Down syndrome), that are known to accelerate the development of PVOD are present.[11] Without intervention, reversal of flow may happen in early childhood or around puberty, and progression of symptoms may lead to death by the second or third decade of life.[12, 13] Interestingly, adult patients with Eisenmenger syndrome may have a better prognosis compared with those with other causes of pulmonary hypertension.[14]
CausesCauses of Eisenmenger syndrome include the following:
Large, uncorrected cardiac shunt or palliative, surgically created systemic-to-pulmonary shunt for congenital heart diseaseLarge, nonrestrictive VSDNonrestrictive PDAAtrioventricular septal defect, including a large ostium primum ASD without a ventricular componentAortopulmonary windowPalliative, surgically created systemic-to-pulmonary anastomosis for treatment of congenital heart diseasePreviousNextPrognosisEisenmenger syndrome is uniformly fatal; however, some patients survive into the sixth decade of life. The usual life expectancy of a patient with Eisenmenger syndrome is 20-50 years if the syndrome is diagnosed promptly and treated with vigilance. The onset of pulmonary hemorrhage is usually the hallmark of a rapid progression of the disease.[15]
The complications of chronic cyanotic heart disease affect multiple organ systems, including the hematologic, skeletal, renal, and neurologic systems, causing significant morbidity and mortality.
The quality of life is poor in patients with Eisenmenger syndrome because exercise tolerance is extremely limited (due to limited oxygen uptake resulting from an inability to increase pulmonary blood flow) and complications are profound. Poor prognosis is predicted by syncope, elevated-right sided pressures, and hypoxemia.
A study by Salehian et al reported that left ventricular dysfunction (defined as left ventricular ejection fraction [LVEF] [16] A simple echocardiographic score relying on right ventricular and right atrial characteristics was found to predict adverse outcomes in patients with Eisenmenger syndrome that is not associated with complex congenital heart disease.[17]
Uncorrected congenital heart disease with development of Eisenmenger complex portends an insidious progression to near complete physical disability.
PreviousNextOccurrenceThe frequency of pulmonary hypertension and the subsequent development of reversed shunting vary depending on the specific heart defect and operative intervention. Such variations include the following:
Large, nonrestrictive VSD or PDA - Approximately 50% of infants with one of these defects develop pulmonary hypertension by early childhood VSD or PDA and transposition of the great arteries - Forty percent of patients develop pulmonary hypertension within the first year of life Large secundum ASD - The natural history of a large secundum ASD differs in that the 10% of cases that progress to pulmonary hypertension do so more slowly and usually not until after the third decade of life Persistent truncus arteriosus and unrestricted pulmonary blood flow - All patients develop severe pulmonary hypertension by the second year of life Common atrioventricular canal - Almost all patients develop severe pulmonary hypertension by the second year of lifeSurgically created systemic-to-pulmonary shunt - The frequency of pulmonary hypertension varies depending on size and anatomyBlalock-Taussig anastomosis (subclavian artery to pulmonary artery) - Ten percent of patients develop pulmonary hypertensionWaterston (ascending aorta to pulmonary artery) or Potts (descending aorta to pulmonary artery) shunt - Thirty percent of patients develop pulmonary hypertension. PreviousNextMorbidityComplications in Eisenmenger syndrome include the following:
Hematologic complications - These include hyperviscosity syndromes related to secondary erythrocytosis and bleeding diathesesNervous system complications – These include brain abscess, transient cerebral ischemia, thrombotic stroke, and intracerebral hemorrhage Hyperbilirubinemia - Increases the risk of gallstonesHyperuricemia - Can cause nephrolithiasis and secondary goutHypertrophic osteoarthropathy - Causes bone pain and tendernessVision loss - Reports document transient vision loss related to peripheral retinal microvascular abnormalitiesCongestive heart failureDysrhythmiaPulmonary infarction and hemorrhageInfective endocarditisSyncope - The systemic vascular bed is prone to vasodilation and subsequent systemic arterial hypotension, which can cause syncope Sudden deathPreviousNextMortalityPatients with Eisenmenger syndrome usually do not survive beyond the second or third decade. Long-term survival depends on the patient’s age at the onset of pulmonary hypertension and the coexistence of additional adverse features, such as Down syndrome. Survival predominantly depends on right ventricular function. The mortality rate in pregnant patients with Eisenmenger syndrome is reported to be approximately 50%, although it may be higher.
The most frequent terminal event in this syndrome is a combination of hypoxemia and arrhythmia in the setting of rapid increases in pulmonary vascular resistance or decreases in systemic vascular resistance (SVR). Death also commonly results from congestive heart failure, massive hemoptysis, or thromboembolism.[12]
PreviousNextPatient EducationThe following points should be considered in patient education:
Inform patients that diet and weight control are essentialEducate patients to avoid smokingProvide an exercise prescriptionAdvise abstinence from or only moderate intake of alcoholEducate patients about contraception options and pregnancy risk (the mortality rate in pregnant patients with Eisenmenger syndrome is approximately 50%)[18] Contraception by means of tubal ligation (with subacute bacterial endocarditis [SBE] prophylaxis) may be recommendedOral or implantable contraceptives may promote pulmonary infarction through activation of the coagulation cascadeEducate patients about the signs and symptoms of polycythemia and hyperviscosityInform patients about the importance of dental hygieneAdditional resources for patients with pulmonary hypertension can be found at the Pulmonary Hypertension Association Web site.
PreviousProceed to Clinical Presentation , Eisenmenger Syndrome












0 comments:
Post a Comment