Loeffler endocarditis and endomyocardial fibrosis are restrictive cardiomyopathies, defined as diseases of the heart muscle that result in impaired ventricular filling with normal or decreased diastolic volume of either or both ventricles. Systolic function and wall thickness may remain normal, especially early in the disease, as reported by Richardson and associates.[1, 2] Both conditions are associated with eosinophilia.
The associations among eosinophilia, active carditis, and multiorgan involvement were first described by Loeffler in 1936.[3] Pathologic specimens in Loeffler endocarditis show eosinophilic myocarditis, a tendency toward endomyocardial fibrosis and clinical manifestations of thromboembolism, and acute heart failure.
Eosinophilic states that may occur in association with Loeffler endocarditis include hypereosinophilic syndrome, eosinophilic leukemia, carcinoma, lymphoma, drug reactions or parasites, as reported in multiple case series.
Although eosinophilic endocardial disease has been well described, myocardial and vascular damage due to eosinophilic infiltration and degranulation is rarely diagnosed during life, as reported by Oakley et al and others.[4] Herzog et al and Tonnesen et al have proposed that the reason for this situation may be the rapidly fatal evolution of most cases of eosinophilic arteritis and myocarditis.[5, 6] These conditions are usually diagnosed based on postmortem examination and nonspecificity of clinical manifestations, as reported by Kim et al, Isaka et al, and Seshadri et al.[7, 8, 9]
Pathophysiologically, the fibrotic stage of Loeffler endocarditis is very similar to the disease entity described as endomyocardial fibrosis, which is indolent in comparison to Loeffler endocarditis. The tropical form of endomyocardial fibrosis is associated with eosinophilia, a common finding in Loeffler endocarditis.
NextPathophysiologyEndomyocardial damage in Loeffler endocarditis is well known and described in a study by Solley and associates.[10] Myocardial involvement is less well known and has been considered a manifestation of an acute necrotic stage of eosinophilic endomyocardial disease, as reported by Olsen and colleagues.[11] More recently, cases of isolated eosinophilic myocarditis have been reported without signs of endomyocardial involvement, with or without vasculitis.
Additionally, idiopathic eosinophilic endomyocarditis, in the absence of peripheral eosinophilia, has been reported by Priglinger et al.[12]
Morphologic abnormalities of eosinophils have been noted in patients with Loeffler endocarditis, suggesting that these eosinophils were mature or stimulated. The intracytoplasmic granular content of activated eosinophils is thought to be responsible for the toxic damage to the heart, as reported by Tai and associates.[13] Spry et al reported eosinophilic degranulation of basic proteins causing myocardial damage in tissue cultures in vitro.[14] Gliech et al reported a dose-dependent cytotoxic effect of the eosinophilic granular proteins, inhibiting multiple enzyme systems.[15]
The cationic eosinophilic proteins bind to the anionic endothelial protein, thrombomodulin. This complex impairs anticoagulant activities, leading to enhanced endocardial thrombus formation, as reported by Slungaard and colleagues.[16]
Toxins released by the eosinophils include eosinophil-derived neurotoxin, cationic protein, major basic protein, reactive oxygen species, and arachidonic acid derivatives. As described by Cunningham et al, these toxins may cause endothelial and myocyte damage, resulting in thrombosis, fibrosis, and infarction.[17]
The intensity and timing of the active carditis is related closely to the severity of the circulating eosinophilia. Some have suggested that, particularly in the tropics, patients who present with later fibrotic stages of endomyocardial disease may have had either transient earlier bouts of moderate eosinophilia with spontaneous resolution, or only moderate levels of eosinophilia leading to a low-grade endomyocarditis with gradual progressive fibrosis, as reported by Olsen et al.[11]
Molecular pathophysiologyCools et al reported a landmark finding by treating patients with hypereosinophilic syndrome (HES) with imatinib, a tyrosine kinase inhibitor.[18]
The gene defect is localized to an interstitial chromosomal deletion on chromosome band 4q12, resulting in fusion of the Fip1-like1 (FIP1L1) gene to the platelet-derived growth factor gene alpha (PDGFRA). The protein product of this gene is a tyrosine kinase enzyme that transforms the hematopoietic stem cells. This FIP1L1-PDGFRA fusion gene defect was identified in 9 of 16 patients treated with imatinib. This study also highlights the importance of reclassifying HES as a myeloproliferative disorder of a possible single clone based on genotyping, as the FIP1L1-PDGFRA gene rearrangement is a clonal abnormality. Treatment with imatinib caused rapid regression of eosinophilic proliferation and endomyocardiopathy in subsequent cases reported by Vandenberghe et al and Rotoli et al.[19, 20]The following list summarizes the initial clinical presentations of eosinophilic endomyocardial disease in relation to the predominant pathologic stage of the disease as reported by Alderman et al in the Textbook of Cardiovascular Medicine.[21] Death is usually related to multiorgan dysfunction in the presence of congestive heart failure. (See Medscape's Heart Failure Resource Center.)
The initial clinical presentation and stages of eosinophilic endomyocardial disease are as follows:[21]
Necrotic stage (early stage) Hypereosinophilia with systemic illness (20-30%) FeverSweatingChest pain (as described by Bestetti et al[22] ) LymphadenopathySplenomegalyAcute carditis (20-50%) AnorexiaWeight lossCoughPulmonary infiltratesSkin and retinal lesionAtrioventricular valve (AV) valve regurgitationBiventricular failurePolymorphic ventricular tachycardia[23] Thrombotic stage Thrombotic emboli (10-20%) Cerebral, splenic, renal, and coronary infarctionSplinter hemorrhagesFibrotic stage (late stage) Restrictive myopathy (10%) AV valvular regurgitationRight and left heart failureThe image shows dense fibrosis of ventricle in a postmortem dissected heart.
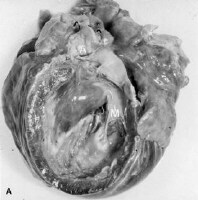 Myocardial as well as valvular involvement with Loffler endocarditis. This image shows dense fibrosis of ventricle in a postmortem dissected heart. PreviousNextEpidemiologyFrequencyUnited States
Myocardial as well as valvular involvement with Loffler endocarditis. This image shows dense fibrosis of ventricle in a postmortem dissected heart. PreviousNextEpidemiologyFrequencyUnited StatesThe condition is rare and is seen mostly in immigrants from Africa, Asia, and South America.
InternationalLoeffler endocarditis is primarily confined to the rain forest (tropical and temperate) belts of Africa, Asia, and South America.
Mortality/MorbidityThe literature reports a 35-50% 2-year mortality rate in patients with advanced myocardial fibrosis. Substantially better survival rates may be seen in less symptomatic patients who have milder forms of the disease. As noted, this rate may reflect underdiagnosis of clinically inapparent disease, as for other types of cardiomyopathy.
RaceThe condition has a predilection for African and African American populations, notably the Rwanda tribe in Uganda, and for people of low socioeconomic status. Whether this is due to genetic factors or the epidemiology of underlying environmental factors is not known.
SexLoeffler endocarditis has a predilection for males. However, endomyocardial fibrosis, which has similar clinical manifestations, is found equally frequently in both sexes.
AgeThe reported age range is 4-70 years. Loeffler endocarditis particularly affects young males, as does its close counterpart, endomyocardial fibrosis, which is more common in children and young adults.
PreviousProceed to Clinical Presentation , Loeffler Endocarditis











0 comments:
Post a Comment