Congenitally corrected transposition of the great arteries (CCTGA) is a rare congenital heart defect in which the heart twists abnormally during fetal development and the ventricles are reversed.
Essential update: Risk factors for patients with systemic right ventricleIn a study of 88 patients with systemic right ventricle (28% with congenitally corrected transposition of the great arteries) who were followed for a mean of 4.3 years, researchers found that patients with a right ventricular end-diastolic volume index >150 ml/m2 and peak exercise systolic blood pressure [1]
Signs and symptomsSymptoms usually reflect associated cardiac anomalies. The most common presenting features include the following:
bradycardia related to high-degree AV heart blocka single loud second heart sound, which is often palpable to the left of the sternum, arising from the anteriorly positioned aortic valve heart murmur due to associated ventricular septal defect, pulmonic stenosis, or tricuspid regurgitationcyanosisheart failuretachyarrhythmiaSee Clinical Presentation for more detail.
DiagnosisThis condition is usually diagnosed later in childhood or in early adult life when patients present with complete heart block or heart failure due to right ventricular decompensation or systemic tricuspid valve regurgitation.
Diagnosis may require some or all of the following tests:
EchocardiogramChest radiographyTransesophageal echocardiographyCardiac MRIElectrocardiographyEchocardiogram and cardiac MRI are most commonly used in the diagnosis of CCTGA.
See Workup for more detail.
ManagementMedical care
There is little evidence that established medical treatment options for left ventricle dysfunction (ACE inhibitors, beta-blockers, nitrates) produce similar outcomes for systemic right ventricles. Caution should be used with administration of beta-blockers, as complete heart block may be precipitated in these patients with known conduction system abnormalities. Ultimately, patients with failing systemic ventricular function may best be served by cardiac transplantation.
Surgical care
For patients that need surgery the type of operation will vary according to the associated defects. There are several options available including the following:
Ventricular septal defect closure (VSD) and insertion of a tube (conduit) between the heart and the lungsTricuspid valve replacementSwitch procedures, including double switch and the Rastelli procedureEarly pacemaker placement is recommended in the setting of complete heart block either during or after surgical intervention or if any significant associated defect, such as cardiomegaly, decreased right ventricular function, symptomatic bradycardia, or heart failure, is present.
See Treatment and Medication for more detail.
Image library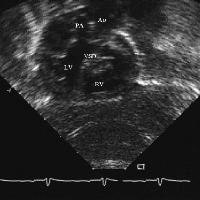 Subcostal view of a 1-year-old child with L-transposition of the great arteries, valvular and subvalvular pulmonic stenosis, and a moderate outlet ventriculoseptal defect (VSD). Note the ventriculoarterial discordance. Note the posterior, rightward position of the pulmonary artery. [PA = pulmonary artery, LV = left ventricle, RV = right ventricle]. NextBackground
Subcostal view of a 1-year-old child with L-transposition of the great arteries, valvular and subvalvular pulmonic stenosis, and a moderate outlet ventriculoseptal defect (VSD). Note the ventriculoarterial discordance. Note the posterior, rightward position of the pulmonary artery. [PA = pulmonary artery, LV = left ventricle, RV = right ventricle]. NextBackgroundCongenitally corrected transposition of the great vessels is a rare congenital heart defect associated with multiple cardiac morphological abnormalities and conduction defects.
PreviousNextPathophysiologyDuring embryological development, left-handed looping of the heart tube results in atrioventricular (AV) discordance, and the aortopulmonary septum fails to rotate 180°, resulting in ventriculoarterial discordance. Blood flows in an effective sequence, hence the name corrected; however, the right ventricle supports the systemic circulation in this disorder.
Venous blood returns from the body into the right atrium before passing through the mitral valve into a morphological left ventricle. Blood then enters the lungs via the pulmonic valve into the main pulmonary artery. Pulmonary venous blood returns to the left atrium and then passes through the tricuspid valve to the morphological right ventricle, exiting to the aorta via the aortic valve. The aorta is positioned anterior and to the left of the pulmonary artery. In effect, the ventricles are transposed.
PreviousNextFrequencyUnited StatesData from the Baltimore-Washington Infant Study supported the fact that congenitally corrected transposition is a rare disorder.[2] As many as 40 infants per 100,000 live births are affected by congenitally corrected transposition of the great vessels; this is fewer than 1% of all congenital heart defects.
InternationalThis disorder is reported in 0.5% of patients with congenital heart disease, and the literature reports fewer than 1000 cases. Most pediatric cardiologists have seen multiple cases of congenitally corrected transposition of the great vessels; however, the true prevalence of the malformation is not known.
PreviousNextMortality/MorbidityTen-year survival rate ranges from 64-83% from the time of diagnosis and is dependent on associated anomalies.Freedom[3] reported an operative mortality rate of 6% and a 15-year actuarial survival rate of 48% in a cohort of patients with congenitally corrected transposition of the great vessels at the Hospital for Sick Children in Toronto. A rare patient without associated cardiac anomalies may have a much more benign course, and literature documents many examples of these patients being diagnosed in the sixth and seventh decades of life.[4, 5, 6] A median age at death of 40 years has been reported in both patients who have undergone operation and those who have not.PreviousProceed to Clinical Presentation , Congenitally Corrected Transposition












0 comments:
Post a Comment