The most common primary cardiac tumor is the atrial myxoma, which accounts for 40-50% of all these neoplasms.[1] The remainder of the pathological spectrum includes benign and malignant cell types. Although the overall incidence of primary cardiac neoplasms is low (0.0001-0.5% in autopsy series), these cardiac tumors provide unique diagnostic and therapeutic challenges.[2, 3, 4]
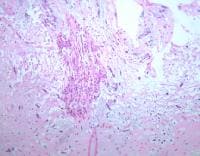 Low-power photomicrograph of cardiac myxoma (hematoxylin and eosin stain).
Low-power photomicrograph of cardiac myxoma (hematoxylin and eosin stain). 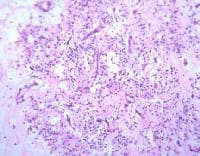 High-power photomicrograph showing the histology of cardiac myxoma (hematoxylin and eosin stain). Note the dark staining polygonal cells characteristic of the tumor.
High-power photomicrograph showing the histology of cardiac myxoma (hematoxylin and eosin stain). Note the dark staining polygonal cells characteristic of the tumor. The clinical symptoms caused by cardiac tumors are generally secondary to their mass effect, local invasion, embolization, or constitutional symptoms. An intracardiac tumor mass may obstruct blood flow, compromise valve function, or induce neurological catastrophe secondary to tumor embolization. The location of the tumor determines the type of symptoms produced, which can include syncope, angina, dyspnea, edema, ascites, depression of pump function, cardiomyopathy, and pulmonary hypertension. Some tumors produce no symptoms and are found incidentally as a consequence of secondary symptoms such as stroke or evidence of peripheral embolization.
Most benign tumors can be resected completely with excellent outcomes. Consider heart transplantation in those instances in which the benign tumor is too large to resect. Resection is the treatment of choice for malignant cardiac tumors; however, long-term results are dismal, even with the addition of adjuvant therapy.[5]
NextPathophysiologySeveral types of tumors can arise in the heart, depending upon the tissues and structures involved. Primary neoplasms may arise from endocardium, valvular structures, primitive tissue rests, and the conduction system. Secondary or metastatic neoplasms arise from hematologic spread of the originating tissue. The physiologic derangements induced by the tumor are dependent upon the location of the mass and the tissue from which it arises.
PreviousNextEpidemiologyFrequencyUnited StatesIncidence depends upon tumor cell type. Overall incidence of the disease is 0.0001-0.5% in autopsy series. Myxomas account for 40-50% of primary cardiac tumors in patients aged 30-60 years.
InternationalRates of cardiac tumors in other countries parallel rates in the United States.
Mortality/MorbidityMyxomas: The mortality rate of patients after myxoma removal does not differ significantly from that of the general population.Rhabdomyoma, fibroma, fibroelastoma, hemangioma, lipoma, teratoma, and hamartoma: These are benign tumors, and mortality rates in patients with these tumors do not differ significantly from that of the general population. Malignant tumors: These tumors are generally sarcomatous in nature. In spite of resections (complete or incomplete), median survival duration ranges from 10-24 months. RacePrimary cardiac tumors appear to occur equally in all races, unless their presence is connected directly with underlying genetic disorders that demonstrate a race predilection.
SexThe frequencies of these tumors in males and females are the same.
AgeCardiac tumors can occur in all age groups.
Cardiac myxoma, lipomatous septal hypertrophy,[6] paraganglioma, and sarcoma tumors occur primarily in adults. Rhabdomyoma, fibroma, teratoma, hamartoma, and Purkinje tumors occur primarily in children.[7] Papillary fibroelastoma,[8] hemangioma, and lipoma occur in all age groups. PreviousProceed to Clinical Presentation , Primary Cardiac Neoplasms












0 comments:
Post a Comment