Third-degree atrioventricular (AV) block, also referred to as third-degree heart block or complete heart block, is a disorder of the cardiac conduction system where there is no conduction through the atrioventricular node (AVN). Therefore, complete dissociation of the atrial and ventricular activity exists.[1] The ventricular escape mechanism can occur anywhere from the AVN to the bundle-branch Purkinje system.[2]
It is important to realize that not all patients with AV dissociation have complete heart block. For example, patients with ventricular tachycardia have AV dissociation, but not complete heart block; in this example, AV dissociation is due to the ventricular rate being faster than the intrinsic sinus rate. On electrocardiography (ECG), complete heart block is represented by QRS complexes being conducted at their own rate and totally independent of the P waves (see the image below).
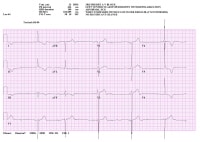 Electrocardiogram from patient in complete heart block.
Electrocardiogram from patient in complete heart block. AV block results from various pathologic states causing infiltration, fibrosis, or loss of connection in portions of the healthy conduction system. Third-degree AV block can be either congenital or acquired. (See Etiology.)
Initial triage of patients with complete heart block consists of determining symptoms, assessing vital signs, and looking for evidence of compromised peripheral perfusion. In particular, the physical examination findings of patients with third-degree AV block will be notable for bradycardia, which can be severe. (See Clinical.)
Treatment of third-degree AV block is based on the level of the block. The first, and sometimes most important, medical treatment for heart block is the withdrawal of any potentially aggravating or causative medications. Medical treatment of complete heart block is limited to patients with conduction disease in the AVN. (See Treatment.)
Initial treatment efforts should focus on assessing the need for temporary pacing and initiating the pacing. Most patients whose heart block is not otherwise treatable will require a permanent pacemaker or an implantable cardioverter defibrillator (ICD).
NextPathophysiologyIn the heart, normal impulse initiation begins in the sinoatrial node. The excitation wave then travels through the atrium. During this time, surface ECG recordings show the P wave. Following intra-atrial conduction to the area of the lower intra-atrial septum, this wavefront reaches the inputs to the AVN. The AVN then conducts the impulse to the His bundle. The His bundle divides into the right and left bundles, which distribute this impulse to the ventricles.
During atrial, AVN, and His-Purkinje conduction, the PR segment is observed. Heart block occurs when slowing or complete block of this conduction occurs. Traditionally, AV block can be divided into first-, second-, and third-degree block.
First-degree AV blockFirst-degree AV block is a condition in which a 1:1 relationship exists between P waves and QRS complexes, but the PR interval is longer than 200 msec. Thus, first-degree AV block represents delay or slowing of conduction. Occasionally, first-degree AV block may be associated with other conduction disturbances, including bundle-branch block and fascicular blocks (bifascicular or trifascicular block).
Second-degree AV blockSecond-degree AV block exists when more P waves than QRS complexes are seen on the ECG, but a relationship between P waves and QRS complexes still exists. In other words, not all P waves are followed by QRS complexes (conducted). Traditionally, this type of AV block is divided into 2 main subcategories, Mobitz type I (Wenckebach) and Mobitz type II.
In the Mobitz I second-degree AV block, the PR interval prolonging until the P wave is not followed by a QRS complex. In a typical Mobitz I block, the PR interval prolongation from beat to beat is greatest in the first interval and progressively less with subsequent intervals. This is reflected in shortening of the R-R interval and the overall PR interval increases. Also, the R-R interval enveloping the pause is less than twice the duration of the first R-R interval following the pause.
On the ECG tracing, Mobitz I second-degree AV block results in the characteristic appearance of grouping beats; conversely, the presence of grouped beating should prompt a careful evaluation for Wenckebach conduction (though it should be noted that not all such conduction is pathologic).
In Mobitz II second-degree AV block, the PR interval is constant, but occasional P waves are not followed by the QRS complexes (nonconducted). Occasionally, the first PR interval following nonconducted P waves may be shorter by as much as 20 msec.
To differentiate between Mobitz I block and Mobitz II block, at least 3 consecutive P waves must be present in the tracing. If only every other P wave is conducted (2:1), a second-degree block cannot be classified into either of these categories and thus is best described as a 2:1 AV block, unless the mechanism can be inferred from surrounding patterns of atrial-to-ventricular conduction.
An AV block resembling second-degree AV block has been reported with sudden surges of vagal tone associated with cough, hiccups, swallowing, carbonated beverages, pain, micturition, or airway manipulation in otherwise healthy subjects. The distinguishing feature is simultaneous slowing of the sinus rate. This condition is paroxysmal and benign but must be carefully differentiated from a true second-degree AV block because the prognosis is very different.
Third-degree AV blockThird-degree AV block (ie, complete heart block) exists when there are more P waves than QRS complexes and there is no relationship between them (ie, no conduction). The conduction block may be at the level of the AVN, the bundle of His, or the bundle-branch Purkinje system. In most cases (approximately 61%), the block occurs below the His bundle. Block within the AV node accounts for approximately one fifth of all cases, whereas block within the His bundle accounts for slightly fewer than one fifth of all cases.[2]
The duration of the escape QRS complex depends on the site of the block and the site of the escape rhythm pacemaker. Pacemakers above the His bundle produce a narrow QRS complex escape rhythm, whereas those at or below the His bundle produce a wide QRS complex.
When the block is at the level of the AVN, the escape rhythm generally arises from a junctional pacemaker with a rate of 45-60 beats/min. Patients with a junctional pacemaker frequently are hemodynamically stable, and their heart rate increases in response to exercise and atropine. When the block is below the AVN, the escape rhythm arises from the His bundle or the bundle-branch Purkinje system at rates slower than 45 beats/min. These patients generally are hemodynamically unstable, and their heart rate is unresponsive to exercise and atropine.
AV dissociationAV dissociation is present when atrial and ventricular activation are independent of each other. It can result from complete heart block or from physiologic refractoriness of conduction tissue. It can also occur in a situation when the atrial/sinus rate is slower than the ventricular rate (eg, with accelerated junctional tachycardia and ventricular tachycardia).
Occasionally, the atrial and ventricular rates are so close that the tracing would suggest normal AV conduction; only careful examination of the long rhythm strip may reveal a variation in PR interval. This form of AV dissociation is called isorhythmic AV dissociation. Maneuvers or medications resulting in acceleration of atrial/sinus rate will result in restoration of normal conduction.
PreviousNextEtiologyAV block results from various pathologic states causing infiltration, fibrosis, or loss of connection in portions of the healthy conduction system. Third-degree AV block can be either congenital or acquired.
The congenital form of complete heart block usually occurs at the level of the AVN. Patients are relatively asymptomatic at rest but later develop symptoms because the fixed heart rate is not able to adjust for exertion. In the absence of major structural abnormalities, congenital heart block is often associated with maternal antibodies to SS-A (Ro) and SS-B (La).[3]
The common causes of acquired AV block are as follows:
Drugs (see below)Degenerative diseases – Lenègre disease (sclerodegenerative process involving only the conduction system) and Lev disease (calcification of the conduction system and valves), noncompaction cardiomyopathy, nail-patella syndrome, mitochondrial myopathy[4] Infectious causes - Lyme borreliosis (particularly in endemic areas), Trypanosoma cruzi infection,[5] rheumatic fever, myocarditis, Chagas disease, Aspergillus myocarditis, varicella-zoster virus infection,[6] valve ring abscess Rheumatic diseases - Ankylosing spondylitis, Reiter syndrome, relapsing polychondritis, rheumatoid arthritis, sclerodermaInfiltrative processes - Amyloidosis, sarcoidosis, tumors, Hodgkin disease, multiple myelomaNeuromuscular disorders - Becker muscular dystrophy, myotonic muscular dystrophyIschemic or infarctive causes - AVN block associated with inferior wall myocardial infarction (MI), His-Purkinje block associated with anterior wall MI (see below)Metabolic causes - Hypoxia, hyperkalemia, hypothyroidismToxins – “Mad†honey (grayanotoxin), cardiac glycosides (eg, oleandrin), and othersPhase IV block (also known as bradycardia-related block)Iatrogenic causes (see below)DrugsComplete heart block can develop from isolated single-agent overdose or—as is often the case—from combined or iatrogenic coadministration of AV nodal, beta-adrenergic, and calcium channel blocking agents. Drugs or toxins associated with heart block include the following:
Class Ia antiarrhythmics (eg, quinidine, procainamide, disopyramide)Class Ic antiarrhythmics (eg, flecainide, encainide, propafenone)Class II antiarrhythmics (beta-blockers)Class III antiarrhythmics (eg, amiodarone, sotalol, dofetilide, ibutilide)Class IV antiarrhythmics (calcium channel blockers)Digoxin or other cardiac glycosides; patients who are on digoxin should be educated about possible early symptoms of digoxin toxicity Myocardial infarctionAnterior wall MI can be associated with an infranodal complete AV block; this is an ominous finding. Complete heart block develops in slightly less than 10% of cases of acute inferior MI and is much less dangerous, often resolving within hours to a few days.
Studies suggest that AV block rarely complicates MI.[7, 8] With an early revascularization strategy, the incidence of AV block decreased from 5.3 to 3.7%. Occlusion of each of the coronary arteries can result in development of conduction disease despite redundant vascular supply to the AVN from all coronary arteries.
Most commonly, occlusion of the right coronary artery (RCA) is accompanied by AV block. In particular, the proximal RCA occlusion has a high incidence of AV block (24%) because there is involvement not only of the AV nodal artery is involved but also of the right superior descending artery, which originates from the very proximal part of the RCA.
In most cases, AV block resolves promptly after revascularization, but sometimes the course is prolonged. Overall, the prognosis is favorable. AV block in the setting of occlusion of the left anterior descending artery (particularly proximal to the first septal perforator) has a more ominous prognosis and usually calls for pacemaker implantation. Second-degree AV block associated with bundle-branch block and in particular with alternating bundle-branch block is an indication for permanent pacing.
IatrogenesisAV block may be associated with aortic valve surgery, septal alcohol ablation, percutaneous coronary intervention to the left anterior descending artery, or ablation of the slow or fast pathway of the AVN. Placement of catheters that mechanically interfere with one fascicle when conduction is already impaired in the remaining conduction system (eg, bumping the right bundle with a pulmonary artery catheter in a patient with existing left bundle-branch block) almost always resolves spontaneously.
AV block after cardiac surgery is seen in 1-5.7% of patients.[9] Major risks factors identified for the need for permanent pacing are aortic valve surgery, preexisting conduction disease (either right or left bundle-branch block), bicuspid aortic valve, annular calcification, and female gender. The time course for recovery varies widely, with a significant portion of patients recovering during the 48 hours following surgery. Available evidence suggests that if no recovery in AV conduction is seen by postoperative day 4 or 5, a pacemaker should be implanted.
PreviousNextEpidemiologyIn the United States, the prevalence of third-degree AV block is 0.02%. Worldwide, the prevalence of third-degree AV block is 0.04%.[10]
The incidence of AV conduction abnormalities increases with advancing age, resembling the age-related incidence of ischemic heart disease. An early peak in incidence occurs in infancy and early childhood due to congenital complete AV block, which is sometimes not recognized until childhood or even adolescence.
PreviousNextPrognosisPatients with complete heart block are frequently hemodynamically unstable, and as a result, they may experience syncope, hypotension, cardiovascular collapse, or death. Other patients can be relatively asymptomatic and have minimal symptoms other than dizziness, weakness, or malaise.
Third-degree AV block may be an underlying condition in patients who present with sudden cardiac death. The cause of death may often be tachyarrhythmias precipitated by the secondary changes in ventricular repolarization (QT prolongation) secondary to the abrupt changes in rate.
Some patients may develop polymorphic ventricular tachycardia when significant bradycardia is present. This is related to prolongation of repolarization with extremely slow rates. This mechanism is also mostly responsible for death in these patients.
When treated with permanent pacing, the prognosis is excellent. The complications related to pacemaker insertion are rare (
PreviousProceed to Clinical Presentation , Third-Degree Atrioventricular Block











0 comments:
Post a Comment