General recommendations and organism-specific therapeutic regimens for myocarditis are provided below, including those for viral[1, 2, 3, 4] and bacterial organisms.[2, 3, 5] Special considerations are also discussed.
General recommendationsMost cases of myocarditis are post viral in origin[6, 7] ; therefore, supportive therapy is first-line treatment.[2]
Obtain hemodynamic stability with vasopressors and inotropic agents, if needed.
Use diuretics and vasodilators if high ventricular filling pressures are noted on echocardiography.
Consider a left ventricular assist device, transplantation, or both in patients with severe disease.
Once the patient is stabilized, follow the American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the treatment of heart failure.[1] Angiotensin-converting enzyme inhibitors (ACEIs), beta-blockade, and an aldosterone antagonist are recommended if the patient has New York Heart Association (NYHA) grade III-IV symptoms).[3, 5]
Diagnostic criteriaEndomyocardial biopsy is the criterion standard for diagnosis of myocarditis.[2, 8, 9]
Historically, the Dallas criteria have been used for histologic diagnosis, although their utility is questioned.
Elevated troponin I (>0.1 ng/mL) is highly specific for the diagnosis of myocarditis; the creatine kinase–muscle-brain (CK-MB) fraction and the total creatine kinase (CK) level are not useful.
Echocardiography is recommended as the initial imaging test of choice in suspected myocarditis.
Cardiac magnetic resonance imaging (MRI) is useful to differentiate between myocarditis and other cardiomyopathies, as well as to target endomyocardial biopsy sites.
Etiological classificationThe classification of myocarditis based on etiology is shown in the chart below.[2, 8, 9]
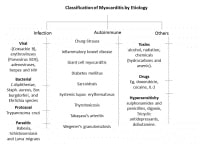 Classification of myocarditis by etiology. Infectious causes and therapeutic guidelines
Classification of myocarditis by etiology. Infectious causes and therapeutic guidelinesViral:
Human immunodeficiency virus (HIV): Initiate antiretroviral therapy; for more information, see Antiretroviral Therapy for HIV InfectionCytomegalovirus (CMV):
Induction therapy: Ganciclovir 5 mg/kg IV q12h for 7-14dMaintenance therapy: Valganciclovir 900 mg PO q24hDuration of therapy: Indefinite, but it may be stopped if the CD4 count is >100 for 6 months[10] Bacterial:Borrelia burgdorferi:
First-degree atrioventricular (AV) block:
Doxycycline 100 mg PO q12h orAmoxicillin 500 mg PO q8h orCefuroxime 500 mg PO q12hDuration of therapy: 14-21dSymptomatic, second- or third-degree AV block:
Ceftriaxone 2 g/day IV orCefotaxime 2 g IV q8hDuration of therapy: 14-28 days[4]Mycoplasma pneumoniae:
Doxycycline 100 mg PO q12h orAzithromycin 500 mg PO q24h orLevofloxacin 500 mg IV or PO q24h orMoxifloxacin 400 mg PO q24h orErythromycin 250 mg PO q6hDuration of therapy: 14-21dMethicillin-resistant Staphylococcus aureus (MRSA):
Vancomycin 15-20 mg/kg/dose IV q8-12h (not to exceed 2 g/dose) (A-II) orDaptomycin 6 mg/kg/dose IV once daily (A-I) for at least 2-6 weeks[11]Corynebacterium diphtheriae:
Erythromycin 40 mg/kg/day PO/IV in divided doses for 14 days; not to exceed 2 g/day orPenicillin G procaine 600,000 U IM for 14d; if weight [12] Parasite:Babesiosis:
Atovaquone 750 mg PO q12h plus azithromycin 500-1000 mg PO on day 1, then 250 mg once daily for 7-10d orClindamycin 300-600 mg IV q6h or 600 mg PO q8h plus quinine 650 mg PO q6-8h for 7-10 days Clindamycin and quinine should be given for those with severe babesiosis[4]Schistosoma mansoni, Schistosoma haematobium, Schistosoma intercalatum:
Praziquantel 20 mg/kg PO for 2 doses within 1 day[13, 14] Protozoa:Trypanosoma cruzi:
Benznidazole 5-7 mg/kg/day PO in 2 divided doses for 60 days (investigational in the United States; available from the CDC)Nifurtimox 8-10 mg/kg/day PO in 3 or 4 divided doses for 90 days[15]Clinical therapeutic considerations for myocarditis scenarios [2, 8, 9, 16]
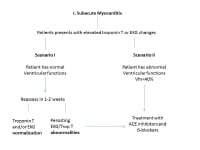
See the acute myocarditis flow chart (first image below) and subacute myocarditis flow chart (second image below).
 Acute myocarditis treatment flowchart.
Acute myocarditis treatment flowchart. 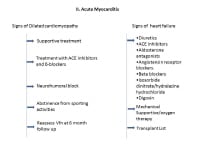 Subacute myocarditis treatment flowchart.
Subacute myocarditis treatment flowchart. Forty percent of dilated cardiomyopathy patients not responding to treatment have myocarditis.[17, 18]
Ten percent of unexplained myocarditis cases are post viral in origin.[6, 7]
The prognosis depends on spontaneous complete resolution (acute fulminant myocarditis) or the development to dilated cardiomyopathy.[19, 20]
Inflammation has beneficial effects on clearing the viral particles; hence, immune suppression is not generally recommended.[21]
Infection with enterovirus and adenoviruses could be treated with 6 mIU interferon 3 times a week to reduce the viral load and improve ventricular function during an acute myocarditis episode.[9]
Studies investigating intravenous immunoglobulin (IVIG) therapy in adults with acute myocarditis and acute myopathy have failed to show any type of usefulness in treatment during an acute episode.
In patients with HIV infection, a long-term follow up (at 5 y) with echocardiogram has shown that 8% show dilated cardiomyopathy changes.[22] However, it is unknown if ACEIs and beta-blockers are effective in these patients.
Autoimmune and hypersensitivityGiant cell myocarditis is the only known cause of most fulminant heart failure with ventricular arrhythmias.[23, 24] Immunosuppression and mechanical cardiac support are recommended in this case and, possibly, cardiac transplantation, with a 20-25% recurrence rate post transplantation. Immunosuppression may have beneficial effects to some extent.[25]
Hypersensitivity-related myocarditis often manifests as infiltration with lymphocytes, histocytes, and eosinophil, and sometimes it results in sudden death from complications of myocarditis.
ComplicationsMyopericarditis with acute coronary syndrome is a potential complication. Treat inflammation with colchicine at 2 mg/day PO with stepwise dose reduction, which should improve pericarditis in 3 months; NSAIDs are contraindicated in this condition.[26, 27]
Syncope with ventricular arrhythmia and cardiac block should be treated with hospital admission with continuous echocardiogram monitoring and conservative management, similar to acute arrhythmias.
Cardiogenic shock may require mechanical ventilator support, extracorporal membrane oxygen therapy, and cardiac transplantation.[28, 29]
, Myocarditis Organism-Specific Therapy












0 comments:
Post a Comment