According to the 2011 US Renal Data System (USRDS) data, in the year 2009, hypertensive nephrosclerosis (HN) accounted for 28% of patients reaching end-stage renal disease (ESRD). The rate of ESRD attributed to hypertension has grown 8.7% since the year 2000.[1] Hypertensive nephrosclerosis is reportedly the second most common cause of ESRD in white people (23%) and is the leading cause of ESRD in black people (46%). The histologic effects of nephrosclerosis are demonstrated in the images below.
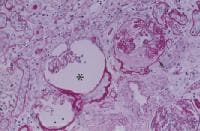 Nephrosclerosis. The glomerular tuft is shrunken, with wrinkling of the capillary walls (asterisk), global glomerular sclerosis (arrow), and complete obliteration of the capillary loops and glomerular ischemia (periodic acid-Schiff stain at 250X magnification).
Nephrosclerosis. The glomerular tuft is shrunken, with wrinkling of the capillary walls (asterisk), global glomerular sclerosis (arrow), and complete obliteration of the capillary loops and glomerular ischemia (periodic acid-Schiff stain at 250X magnification). 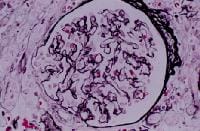 Nephrosclerosis. Glomerulus with wrinkling of glomerular basement membranes accompanied by reduction of capillary lumen diameter (silver stain at 400X magnification).
Nephrosclerosis. Glomerulus with wrinkling of glomerular basement membranes accompanied by reduction of capillary lumen diameter (silver stain at 400X magnification). 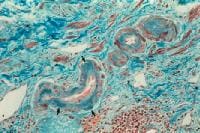 Nephrosclerosis. Hyaline arteriosclerosis with hyaline deposits (arrows) (trichrome stain at 250X magnification).
Nephrosclerosis. Hyaline arteriosclerosis with hyaline deposits (arrows) (trichrome stain at 250X magnification). 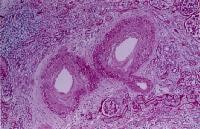 Nephrosclerosis. Fibrointimal proliferation of the arcuate artery (periodic acid-Schiff stain at 150X magnification).
Nephrosclerosis. Fibrointimal proliferation of the arcuate artery (periodic acid-Schiff stain at 150X magnification). The term hypertensive nephrosclerosis has traditionally been used to describe a clinical syndrome characterized by long-term essential hypertension, hypertensive retinopathy, left ventricular hypertrophy, minimal proteinuria, and progressive renal insufficiency. Most cases are diagnosed based solely on clinical findings. In fact, most of the literature dedicated to hypertensive nephrosclerosis is based on the assumption that progressive renal failure in a patient with long-standing hypertension, moderate proteinuria, and no evidence suggesting an alternative diagnosis characterizes hypertensive nephrosclerosis.
The lack of firm criteria on which to base a histologic diagnosis and the lack of a clear demonstration that hypertension initiates the development of renal failure likely indicate that the true prevalence of hypertensive nephrosclerosis has been overestimated. The paradoxical results of increasing incidence of renal failure despite wider antihypertensive drug therapy and reduction in hypertensive target events, such as stroke and cardiovascular disease, raises questions about the causal role of hypertension in this disorder.
As reported by Zuccalà and Zucchelli (1996), part of the confusion in the classification of hypertensive nephrosclerosis stems from the use of the word nephrosclerosis.[2] Coined almost a century ago by Theodor Fahr, nephrosclerosis literally means "hardening of the kidney." In the United States and Europe, the terms hypertensive nephrosclerosis, benign nephrosclerosis, and nephroangiosclerosis are commonly used to describe the same clinical condition. These terms refer more to the renal pathologic changes attributed to the effects of hypertension than to the clinical disorder in question.[3] Unfortunately, the pathologic changes are not specific to hypertensive renal injury; they are also observed in kidney biopsy specimens of patients who are normotensive, particularly those of advanced age or with diabetes.
Unlike morbidity and mortality of stroke and coronary disease, incident cases of ESRD attributed to hypertension continue to increase. Some authors suggest that many of these cases are more likely related to other factors, including small vessel injury related to aging, diabetes, or obesity -related kidney injury.
A couple of important points have been made in different studies. First, among an unselected sample of community-based participants in the Framingham Heart Study, the combination of hypertension and a mild reduction in the glomerular filtration rate (GFR) was found to be an important risk factor for the development of new-onset kidney disease. Other factors noted were diabetes, obesity, smoking, and a low high-density lipoprotein cholesterol level. Second, systolic blood pressure (BP) is a strong, independent predictor of a decline in kidney function among older persons with isolated systolic hypertension. This is a significant finding because most cases of uncontrolled hypertension in the United States are due to systolic hypertension among older adults.
Most patients reaching ESRD from any cause are hypertensive, with nephrosclerosis being the classic finding in end-stage kidneys. Regardless of the etiology, once hypertension develops, a cycle of renal injury, nephrosclerosis, worsening of hypertension, and further renal injury is established. As a result, in a patient presenting with ESRD, determining whether nephrosclerosis is the cause or the consequence of chronic renal injury may be difficult.
NextPathophysiologyTwo pathophysiologic mechanisms have been proposed for the development of hypertensive nephrosclerosis. One mechanism suggests that glomerular ischemia causes hypertensive nephrosclerosis. This occurs as a consequence of chronic hypertension resulting in narrowing of preglomerular arteries and arterioles, with a consequent reduction in glomerular blood flow. Alternatively, glomerulosclerosis occurs because of glomerular hypertension and glomerular hyperfiltration. According to this theory, hypertension causes some glomeruli to become sclerotic. As an attempt to compensate for the loss of renal function, the remaining nephrons undergo vasodilation of the preglomerular arterioles and experience an increase in renal blood flow and glomerular filtration. The result is glomerular hypertension, glomerular hyperfiltration, and progressive glomerular sclerosis. These mechanisms are not mutually exclusive, and they may operate simultaneously in the kidney.
Furthermore, Tracy and Ishii (2000) postulate that nephrosclerosis may not be a single disease entity in the sense of responding to a single etiology, such as hypertension or aging.[4] Rather, nephrosclerosis appears to be multifactorial. It may be, in part, a consequence of fibroplasias in microscopic arteries causing ischemic damage to some nephrons; however, it also may be the end product of a mixture of converging separate pathologic conditions, ie, "second hits," of which only some are known.
Genetically mediated animal models of hypertension, including the Dahl rat and the spontaneous hypertensive rat (SHR), have been used to investigate the role of hypertension in the development of nephrosclerosis. Fundamental differences exist among the strains and between rat and human hypertension. The SHR most closely resembles human essential hypertension. The SHR becomes hypertensive without exposure to salt. Micropuncture studies in hypertensive rats demonstrate an increased preglomerular vasoconstriction that is effective in preventing the development of intraglomerular hypertension. In fact, the SHR develops little renal damage, unless uninephrectomized. In these animals, rigorous BP control does not prevent the development of proteinuria and the pathologic changes of hypertensive nephrosclerosis. The Dahl salt-sensitive rat develops proteinuria before hypertension and before a high-sodium diet is administered.
In patients with primary hypertension, hemodynamic studies frequently show a reduction in renal blood flow. The increased preglomerular vasoconstriction of the afferent arteriole and interlobular artery is thought, at least initially, to exert a protective effect in the glomerulus. With time, sclerosis of the preglomerular vessels causes further reduction in renal blood flow. The GFR is maintained because of increased intraglomerular pressure secondary to efferent arteriolar vasoconstriction and systemic hypertension. Eventually, glomerular ischemia and tubular ischemia develop. Considered together, these data suggest that hypertension precedes and accelerates arteriolar changes in the renal vessels.
Wang et al investigated whether podocyte injury is an important factor in the pathogenesis of hypertensive nephrosclerosis. In a study involving 41 patients with biopsy-proven hypertensive nephrosclerosis, 10 cadaveric kidney donors, and 9 healthy subjects, the authors found that compared with controls, intrarenal messenger ribonucleic acid (mRNA) expression was lower, and urinary mRNA expression was higher, for the podocyte-associated molecules nephrin, podocin, and synaptopodin in patients with hypertensive nephrosclerosis. Moreover, patients with nephrosclerosis had a significantly lower density of glomerular podocytes than did kidney donors (545 +/- 237 vs 773 +/- 296 per glomeruli, respectively; P [5, 6]
GeneticsA genetic link for hypertension and related renal failure is supported by studies demonstrating familial clustering of hypertensive nephrosclerosis in black people and, to some extent, in white people.
In the Multiple Risk Factor Intervention Trial (MRFIT), no changes in the reciprocal creatinine slope were observed in white people, but a significant loss in kidney function was observed in black people despite similar levels of BP control. Similarly, secondary analyses from the Modification of Diet in Renal Diseases (MDRD) study demonstrated that at equivalent mean arterial pressures greater than 98 mm Hg, black patients had a reduction in their GFR at a rate of approximately 1 mL/min/y more than white patients. These observations have led to investigations into genetic factors predisposing to renal damage.
In 2008, 2 separate groups showed strong association between genomic variants within MYH9 (non–muscle myosin heavy chain 9) on 22q and nondiabetic ESRD in African Americans.[7, 8] The 2 other disease entities associated with MYH9 included HIV nephropathy and focal segmental glomerulosclerosis (FSGS) in African Americans.
In 2010, 2 other groups showed an even stronger association between the APOL1 gene and risk of ESRD in African Americans.[9, 10] APOL1, which encodes apolipoprotein L1, is also on 22q and is separated from the MYH9 gene by only 14’000 nucleotides. Two variants of APOL1 that have been associated with increased risk of nephropathy include nonsynonymous coding variants termed G1 (glycine-342 to methionine-384) and in-frame 6bp deletion termed G2. The ApoL1 protein protects against Trypanosoma infection. However, the wild-type ApoL1 protein can be neutralized by Trypanosoma brucei rhodesiense. These 2 gene variants restore immunity to Trypanosoma brucei rhodesiense. As a result, genomic evolution has led to positive selection for APOL1 risk variant.
More recent studies have further shown that nondiabetic carriers of 2 APOL1 variants have a 3-times higher rate of proteinuria and reduced renal function and carriers of 1 or 2 variants are significantly younger at the time of initiation of dialysis.
The African American Study of Kidney disease (AASK) trial evaluated the role of intensive versus standard BP control on progression of kidney disease in 1094 black patients with chronic kidney disease (GFR 20-65 mL/min/SA).[11] The study was done in a trial phase followed by a cohort phase. Overall, no difference was noted in the rate of disease progression in the 2 groups. In the subanalysis, in which patients were stratified based on the degree of proteinuria, patients who had initial urinary protein-to-creatinine ratios of less than 0.22 did not benefit from the intensive BP control, whereas those with urinary protein-to-creatinine ratio of greater than 0.22 benefited from the intensive therapy at the end of the cohort phase. APOL1 and MYH9 nephropathy risk variants have been associated with kidney disease in the AASK participants.[12]
This genetic predisposition may be the reason why tighter control of BP in this black population does not slow the progression of kidney disease. Some authors argue that hypertension in this setting is secondary to underlying renal injury.[13]
In different populations studied regarding polymorphism in the angiotensin-converting enzyme (ACE) gene, the DD genotype is associated with a higher prevalence of progressive renal disease. This genotype is more common in the black population than the white population. Black people with hypertension also have increased angiotensinogen mutations compared with white people with hypertension. Homozygous D polymorphism is associated with an enhanced pressor response to angiotensin I. In patients with immunoglobulin A nephropathy, homozygous D polymorphism appears to influence the rate of progression of renal diseases and the response to ACE inhibitors; thus, ACE polymorphism could be a modulator for the renal response to injury and the response to treatment in persons with hypertensive nephrosclerosis. Whether these data are also applicable to the black population remains to be determined.
Noting that hypertension-associated ESRD displays familial aggregation in the black population, Fung et al investigated possible links between genetic variations and GFR declines. In a study of 554 black patients, the investigators found evidence that such declines can be predicted by variations in the adrenergic beta-1 (ADRB1) receptor at the Ser49Gly position. The authors also found that GFR decline was significantly smaller in patients who were Gly(49)/Gly(49) (minor allele) homozygotes than in those who were Ser(49) carriers.[14]
PreviousNextEpidemiologyFrequencyUnited StatesOver the last 2 decades, ESRD attributed to hypertensive nephrosclerosis has contributed significantly to the increase in new patients starting dialysis in the United States. According to the 2011 USRDS data, the rate of ESRD due to hypertension has grown 8.7% since the year 2000, whereas the rate of ESRD due to glomerulonephritis has fallen 23% and rate of ESRD secondary to diabetes has remained relatively stable. When patients are separated according to race, hypertension is the leading cause of ESRD in black people, accounting for 34% of patients initiating dialysis during this period.
InternationalIn Europe, according to the European Dialysis and Transplant Association registry, hypertensive nephrosclerosis is a less common cause of ESRD, accounting for 12% of new patients starting renal replacement therapy. However, the reported incidence varies among different countries, with France and Italy reporting hypertensive nephrosclerosis as being responsible for ESRD in 25% and 17% of patients starting dialysis, respectively. Whereas in United Kingdom (all countries included), it accounts for 6.1% of patients starting new on dialysis. In Asia, hypertension appears to be a relatively infrequent cause of ESRD, with both Japanese and Chinese registries reporting 6% and 7%, respectively. Establishing whether these differences are real or reflect differences in accuracy of diagnosis or criteria for diagnosis in different countries is difficult.
Mortality/MorbidityAccording to the 2011 USRDS, the annual mortality rate for patients on hemodialysis in the United States is 23.3%. Hypertensive nephrosclerosis accounts for more than one third of patients on hemodialysis.
RaceMarked differences exist in the stated prevalence of hypertensive nephrosclerosis among patients of different ethnic backgrounds. Although black people make up 12% of the US population, they account for 28.3% of the patients on renal replacement therapy. With perhaps the exception of atherosclerotic renal disease, black people are at an increased risk of renal diseases from any cause, especially hypertensive nephrosclerosis. In black people, hypertensive nephrosclerosis occurs earlier, is more severe, and more often causes ESRD (36.8% in black patients vs 26% in white patients).
In persons of all age groups, ESRD is more common in black people; the rate of developing ESRD is 3.5 times higher than the rate found among whites. The increased susceptibility of black patients with hypertension to develop progressive renal failure cannot be explained solely by the higher prevalence of hypertension, severity of hypertension, or socioeconomic factors because the rate of new ESRD cases has remained stable in African Americans, whereas it has grown 7.2% among white, and, in addition, the rates of stroke and cardiovascular mortality have decreased equally in both white and African American populations.
Results from the MRFIT trial indicated that effective BP control was associated with stable renal function in white people but not in black people. In the AASK trial, which specifically evaluated black populations, intensive control of BP in nonproteinuric patients did not decrease progression of kidney disease.
Several renal, hormonal, physiologic, and genetic factors have been proposed as explanations for the increased rate of hypertension and progression of chronic kidney disease in African Americans. These include increased BP sensitivity to high-salt diet, increased renal vascular resistance, decreased renal blood flow, increased tortuosity and occlusion in the interlobular and arcuate arteries based on renal angiograms in African Americans, and decreased nephron mass secondary to low birth weight (more common in African Americans). Lastly, the increased variant in APOL1 gene has been proposed as the cause of the increased rate of ESRD in African Americans.
AgeThe diagnosis of hypertensive nephrosclerosis increases with advancing age. The peak age for the development of ESRD in white patients is 65 years and older, while the peak age is 45-65 years in black people. In most cases, the diagnosis of hypertensive nephrosclerosis in older patients is made clinically because of the reluctance to perform a renal biopsy in this elderly population.[15] Even when a renal biopsy specimen is available, distinguishing vascular lesions due to aging from those due to hypertension may be difficult. In this respect, atheromatous renal vascular disease has been increasingly recognized as a common finding in patients older than 50 years.
Rimmer and Gennari (1993) estimate that atheromatous renal vascular disease accounts for 5-15% of all patients who develop ESRD each year.[16] In addition, cholesterol embolism resulting from atheromatous plaque disruption with subsequent shedding of cholesterol crystals into the renal circulation is frequently diagnosed in this patient population. Both renal artery stenosis and cholesterol embolism are associated with renal microvascular lesions and with glomerular sclerosis. Neither of these findings should be underestimated because patients older than 65 years represent at least 45% of the total population of patients on dialysis in the United States. Similarly, Appel et al (1995) found bilateral renal artery stenoses in 11% of patients on hemodialysis who are older than 50 years.[17] After extrapolating their results to the total number of cases of ESRD, multiplying by the number of patients aged 50 years or older, and multiplying by the number of patients with ischemic renal disease, Appel et al concluded that more than 3500 cases of ischemic renal disease remain undiagnosed each year in the United States.[17] If these predictions are correct, ischemic renal disease is likely the fourth most common cause of ESRD in patients older than 50 years. Hansen et al (2002) provided the first population-based estimate of the prevalence of renovascular disease among free-living elderly American participants of the Cardiovascular Health Study (CHS).[18] This is a multicenter, longitudinal cohort study of cardiovascular disease risk factors, morbidity, and mortality among free-living adults older than 65 years. CHS participants numbered 870, and each underwent renal duplex sonography to assess for the presence or absence of renovascular disease, defined as greater than or equal to 60% diameter-reducing renal artery stenosis or occlusion. The results of this study show that renovascular disease is present in 6.8% of all individuals, regardless of race (6.9% of white participants and 6.7% of black participants). PreviousProceed to Clinical Presentation , Nephrosclerosis












0 comments:
Post a Comment